C19.Life
An archive of scientific studies, articles, resources, and public commentary regarding SARS-CoV-2 – the virus at the heart of COVID-19.
➲
About C19.Life (and you)
2020–2026
❦ on basic degrees of humanity
❦ ‘First do no harm; then try to prevent it.’
Dr. Geoffrey Hughes, MBBS, DRCOG, FFAEM, FRCP, FACEM ➲
❦ an overflight
❦ ‘Without information, there is no informed choice.’
by Zdeněk Vrožin, from “A Raven’s Overview” (2026)
❦ the early SARS-CoV-2 (COVID-19) narrative
‘The narrative that COVID-19 had only respiratory sequelae led to a delayed realization of the neurological, cardiovascular and other multi-system impacts of COVID-19 [SARS-CoV-2 infection].’
Nature Reviews Microbiology (2023) ➲
❦ on not needing to read between the lines
‘Despite the perception that COVID-19 is now a mild disease, there is overwhelming evidence indicating that SARS-CoV-2 infection is capable of producing widespread post-acute sequelae in a significant percentage of infections.
This includes a substantial impact on the nervous system resulting from a combination of direct infection, systemic inflammation, immune dysfunction, vascular complications, and tissue hypoxia.’
Psychiatry and Clinical Neurosciences (2025) ➤


© 2026 SARS-CoV-2 / COVID-19 Genomic Sequence Variant Visualiser by Mike Honey ➲
❦ on playing with SARS viruses
‘The clinical manifestations of COVID-19 [SARS-CoV-2 infection] range from asymptomatic to fatal.
Post-COVID-19 conditions are characterized by multi-organ structural and functional impairment, including cardiovascular, neurological, psychiatric, hematological, pulmonary, and dermatological injury.
Although COVID-19 primarily presents as a respiratory infection with flu-like symptoms, it is now considered a multi-organ disease, often involving the nervous system.
Recent evidence indicates that approximately 80% of people who are infected with COVID-19 have one or more long-term symptoms.’
The Lancet: Regional Health (Western Pacific) (2023) ➤
❦ from lung to multi-organ systems
‘Initially focused on respiratory symptoms, it’s now clear that COVID-19 presents a complex clinical picture affecting various organ systems.
Our findings reveal that a substantial proportion of pediatric COVID-19 patients with neurological symptoms exhibit abnormal neuroimaging findings, with 43.74% of children in the included studies demonstrating such abnormalities.’
Nature Scientific Reports (2024) ➤
❦ on not sparing the children
‘While the respiratory symptoms of COVID-19 have dominated the early narratives of the disease, it has become increasingly clear that the virus’s impact stretches far beyond the lungs.
The pediatric population, once thought to be relatively spared from severe outcomes, has presented with significant neurological manifestations that raise concerns about the short- and long-term effects of SARS-CoV-2 on the developing nervous system.
This points to a potentially troubling legacy of the pandemic – neurological sequelae that could impair children’s cognitive outcomes and quality of life long after recovery from the initial infection.’
Bioengineer / Nature Pediatric Research (2025) ➲
❦ on posterity
‘Regarding the different cognitive functions, our results reveal that attention is the one that shows the greatest deficit, regardless of the age of the patients (more than 25% of patients in each age group exhibit a moderate attention deficit).
Processing speed was also a cognitive process that was impaired relatively homogeneously across age groups; however, the results indicate that the youngest patients show a much slower processing speed (33.3% of those under 50 years of age) compared to the oldest (5.1% of those over 50 years of age).
The highest percentage of patients with severe verbal memory impairment was also found in the younger patients group.
In long-term memory, 20.7% of the youngest group showed a severe deficit and 24.1% a mild impairment, while a minimum proportion of the elderly showed alterations in this area.
In conclusion, the results presented here reveal that at least 85% of the participants exhibit deficits in one neuropsychological test.
Also, the youngest patients were those who showed the most marked and heterogeneous cognitive impairment.’
Nature Scientific Reports (2023) ➤
❦ on excess deaths in middle-aged adults
‘For middle-aged adults (50–64) in England from June 2022 to June 2023, the relative excess for almost all causes of death examined was higher than that seen for all ages.
Deaths involving cardiovascular diseases were 33% higher than expected, while for specific cardiovascular diseases, deaths involving ischaemic heart diseases were 44% higher, cerebrovascular diseases were 40% higher and heart failure was 39% higher.
Deaths involving acute respiratory infections were 43% higher than expected and for diabetes, deaths were 35% higher.
Deaths involving liver diseases were 19% higher than expected for those aged 50–64.
The pattern now is one of persisting excess deaths which are most prominent in relative terms in middle-aged and younger adults, with deaths from CVD [cardiovascular] causes and deaths in private homes being most affected.’
The Lancet: Regional Health (Europe) (2023) ➲

❦ ‘Estimated cumulative excess deaths during COVID-19, World’.
© 2025 OurWorldInData.org ➤ / Additional annotations by C19.Life.
✾ For a full picture, see ‘A WHO’s Who of VOCs, VOIs and VUMs: Alphabet Stew and Numeric Ragout for Dummies’ by C19.Life.
❦ on neonates, maternal SARS-CoV-2 infection, placentitis, and severe outcomes
‘Maternal SARS-CoV-2 infection has been associated with increased adverse events in the mother, as well as increased stillbirths, spontaneous abortions, and premature delivery.
SARS-CoV-2 placentitis is a well-documented outcome of symptomatic and asymptomatic COVID-19 infection during pregnancy.
It can disrupt placental function and lead to severe outcomes in the neonate, including growth restriction and stillbirths.’
Archives of Pathology & Laboratory Medicine (2025) ➤
❦ breathing in: reduced foetal lung growth
‘In pregnant women who tested positive for SARS-CoV-2, normalised fetal lung volume was significantly reduced.
The timepoint of infection showed significant effects on fetal lung growth, with reduced lung volumes observed with SARS-CoV-2 infections acquired during the third trimester.’
The Lancet: Respiratory Medicine (2022) ➤
❦ breathing out: SARS-CoV-2 and foetal brain haemorrhages
‘Strikingly, the [foetal brain] haemorrhages are predominately found in the late first and early second trimester of gestation.
Specifically, the majority were between 12 and 14 PCW [post-conception week], a critical window of human foetal brain development when the endothelial tight junctions increase to form the blood-brain barrier.
Our observations of disrupted foetal cerebral vasculature are consistent with reports of damage to the microvasculature of the adult brain in SARS-CoV-2 infected patients.’
Brain (2023) ➤
On Brain Damage
❦ the continuing SARS-CoV-2 narrative of hand-washing for an airborne virus
SARS-CoV-2 – the virus that causes COVID-19 – is airborne.
In May 2021, the WHO officially recognised that SARS-CoV-2 is primarily and predominantly airborne via microscopic aerosols – meaning that the virus is transmissible through the air at both long and short range.
To extol hand-washing as a primary defence against SARS-CoV-2 infection is about as stupid as promising a two-pack-a-day smoker that the simple formula of soap + water will prevent chronic obstructive pulmonary disease and lung cancer.
❦ on reinfections and SARS-CoV-2
‘Reinfection, which is now the dominant type of SARS-CoV-2 infection, is not inconsequential; it can trigger de novo Long Covid [PASC] or exacerbate its severity.
Each reinfection contributes additional risk of Long Covid [PASC]: cumulatively, two infections yield a higher risk of Long Covid than one infection, and three infections yield a higher risk than two infections.’
Science (2024) ➲
❦ on playing the [long] blame game
‘The main symptoms during the first infection in this Omicron wave were fever and sore throat, while sore throat was the main symptom in the reinfection; the average interval for SARS-CoV-2 [COVID-19] reinfection was 149.91 days.
The reasons for COVID-19 reinfection are multifaceted, primarily including low antibody levels, the shortened duration of immune protection provided by antibodies, the mutation of viral strains, non-adherence to epidemic prevention measures by the population, hesitancy towards vaccination, and public fatigue due to the prolonged pandemic.’
BMC Infectious Diseases (2024) ➤
❦ on reinfections, milder symptoms, and increased severity & incidence of Post-Acute Sequelae of COVID-19 (PASC)
‘While acute [short-term] symptoms of reinfection are generally milder, the severity and incidence rate of long COVID [PASC] increase significantly with the number of reinfections.’
The Lancet: Regional Health (Western Pacific) (2024) ➤
On Reinfections

❦ Durability of XBB.1.5 Vaccines against Omicron Subvariants
‘The [Omicron XBB.1.5] vaccine effectiveness against infection reached a level of 52.2% after 4 weeks. It decreased to 32.6% after 10 weeks, and to 20.4% after 20 weeks.
The effectiveness against hospitalization reached a level of 66.8% after 4 weeks, and decreased to 57.1% after 10 weeks.
The [Omicron] XBB.1.5 vaccines were less protective against [Omicron] JN.1 than against [Omicron] XBB sublineages.’
The New England Journal of Medicine (2024) ➤
❦ on the ‘hybrid immunity’ pipe dream
‘The arrival of the Omicron variant marked a major shift, introducing numerous extra mutations in the spike gene compared with earlier variants.
Before Omicron, natural infection provided strong and durable protection against reinfection, with minimal waning over time.
However, during the Omicron era [late 2021 to the present (February 2026)], protection was robust only for those recently infected, declining rapidly over time and diminishing within a year.’
Nature (2025) ➲
On Vaccination

❦ on vaccine effectiveness
‘Vaccine effectiveness against SARS-CoV-2 infection [COVID-19] declines markedly with time and Omicron variants.’
European Respiratory Review (2025) ➲
❦ ‘Omicron variants’ during the ‘Omicron Era’ (late 2021–).
© 2025 NextStrain.org / GISAID.org ~ Additional annotations by C19.Life. ➲
❦ on lymphocytopenia
‘Patients with HIV infection routinely have lymphocytopenia, which arises from destruction of CD4+ T cells infected with the HIV virus.
Patients with COVID-19 also frequently have lymphocytopenia (35% to 83% of patients).
Patients [with frequent lymphocytopenia] have recurrent viral, bacterial, fungal, or parasitic infections.’
Merck & Co. (Merck Manuals) ➲
❦ on the 12-month immunity tail of mild-to-moderate SARS-CoV-2 infections
‘A positive test for COVID-19 is associated with increased rates of diagnosis of various non-SARS-CoV-2 infections in the 12 months following an acute SARS-CoV-2 infection, even if the initial infection is mild to moderate.
Participants with a positive COVID-19 test who were not admitted had significantly increased rates of outpatient diagnosis of bacterial, fungal, and viral infectious illnesses (increased risk of 17%), outpatient respiratory infections (increased risk of 46%), and admission to hospital for infectious illnesses (increased risk of 41%), including for sepsis and respiratory infections.’
CIDRAP / The Lancet: Infectious Diseases (2025) ➲
❦ on immunological dysfunction, and multi-drug-resistant pathogens
“Reduced immune function after a viral infection is not unusual.
Many viruses do this.
The concerning issue is the length and breadth of the immune system dysfunction, coupled with emerging evidence of other pathogens taking advantage.”
Dr. Noor Bari • Emergency Medicine (2022) ➲
❦ on indiscriminate killing of T cells, immune “reset”, and the reactivation of dormant viruses
‘SARS-CoV-2 is linked to an unusually high level of ‘indiscriminate’ killing of T cells, reminiscent of measles, which can cause immune amnesia by depleting memory B cells (a different type of immune cell), leaving people vulnerable to pathogens they were previously immune to.
This concept of immune “reset” after infections isn’t new.
A hallmark of this phenomenon is the reactivation of dormant viruses which re-emerge, while the immune system is in a weakened state.
Reactivation of viruses, including Epstein-Barr virus [human herpesvirus 4] and varicella zoster virus [human herpesvirus 3 → chickenpox (varicella) → shingles (herpes zoster)], has been commonly observed after COVID-19.’
BMJ (2025) ➤
❦ on the other ‘C-[19]Word’
‘Some viruses are known to be associated with the onset of specific cancers.
These micro-organisms – oncogenic viruses or oncoviruses – can convert normal cells into cancer cells.
Recent research indicates that SARS-CoV-2 infection and COVID-19 progression may predispose recovered patients to cancer onset and accelerate cancer development.’
International Journal of Molecular Sciences (2023) ➲
❦ on naïvety, and neglect of pragmatism
“Because children haven’t been exposed to many viruses, their immune system is still ‘naive’.
And because they don’t develop memory T cells, they are at risk of getting sick when they become reinfected.
With each new infectious [SARS-CoV-2] episode as they get older, there is a risk of their T cells becoming ‘exhausted’ and ineffective, like the T cells in older people.
The price that children pay for being so good at getting rid of the virus in the first place is that they don’t have the opportunity to develop ‘adaptive’ memory to protect them the second time they are exposed to the virus.”
Clinical Immunology / News Medical Life Sciences (2023) ➲
C-19 Archives
❦ A raven’s overview
‘In people with pre-existing dementia, SARS-CoV-2 infection is repeatedly associated with faster cognitive decline.
For families, that can mean the difference between years at home and a rapid fall over months.’
Zdeněk Vrožin (2026) ➲
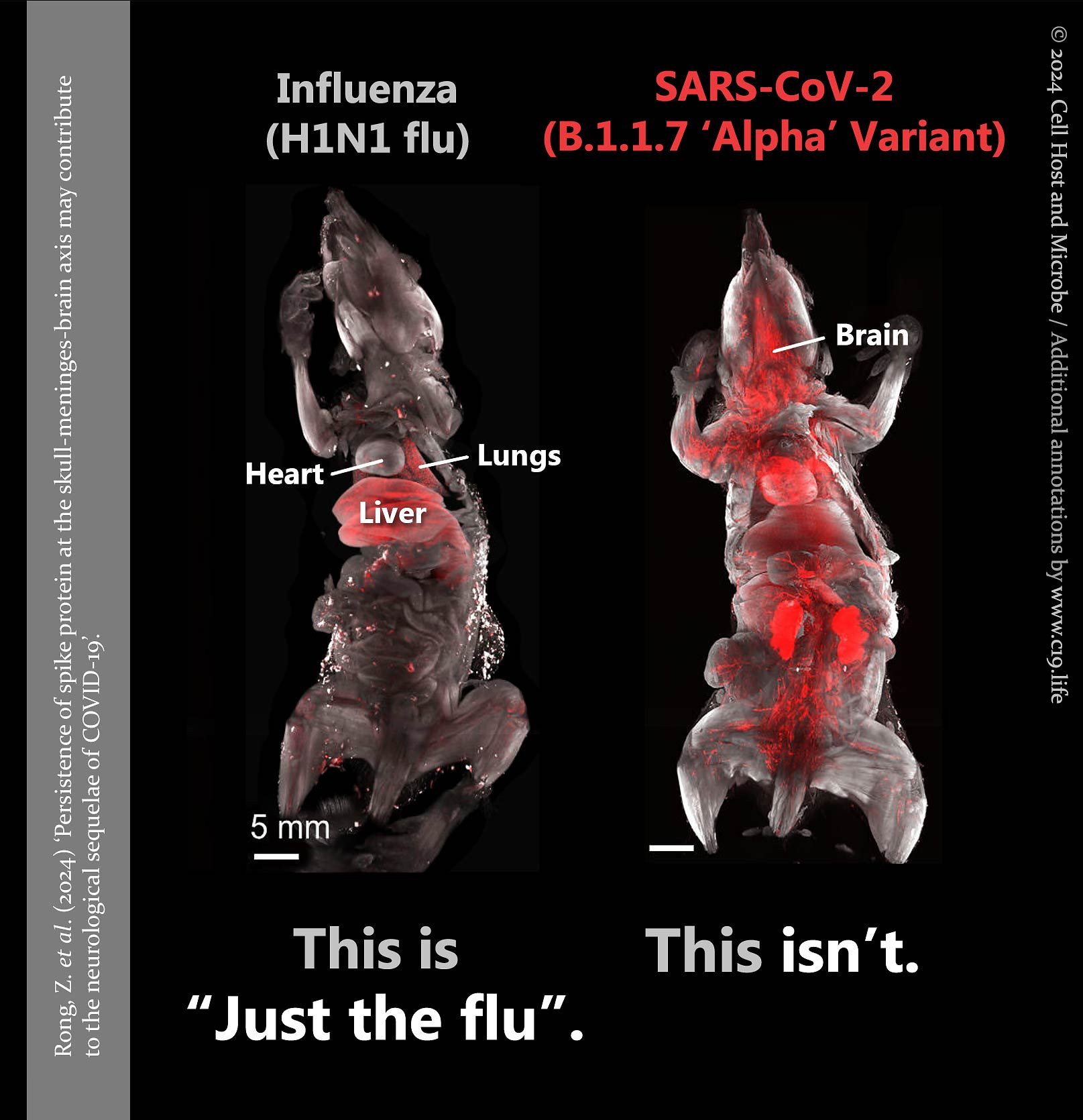
❦ on flu, SARS-CoV-2, and doing your own homework
Now here’s a break from protocol.
If you’re an adult, you will, on average, catch influenza about twice every ten years – or once every five years, which is the norm.
Conservatively, you are catching a fresh SARS-CoV-2 infection about once every year; potentially twice or more annually depending on the variant landscape, your occupation and circumstances, your vaccine history, and the current state of your body.
If you are an average adult – and there’s no reason to believe you aren’t – you will have caught between four and six-plus different strains of SARS-CoV-2 to date [25 Feb 2026].
If you are a child you will have caught, on average, between five and seven-plus SARS-CoV-2 infections to date.
The danger of continuous reinfection is cumulative damage – to your heart and your circulatory system, your brain and nervous system, your immune system, your musculoskeletal system, your integumentary system (which includes your skin and hair), your endocrine system, your respiratory system, your urinary and digestive systems, your reproductive system – and it is up to you to decide how many reinfections you and those around you can take before that damage becomes debilitating, irreversible, and fatal.
This is the time to do your own research – your own homework.
Take a look at the cherry orchard for yourself. (In total, there are 479,424 scientific studies to pick from.)
After all: why believe the gardener?
C19.Life (25 February 2026)
❦ one from the head
‘A bizarre recurring point of debate:
— “People die every day of lots of other things!”
True, but you don’t catch a stroke from other people in a restaurant.’
NHS Palliative Medicine Consultant (2023)
❦ afterword
“The reason why most people aren’t taking Covid-19 seriously is because they simply can’t imagine that their public health body would abandon protections and let an incredibly disabling and airborne virus spread wildly.
They will be very angry when it becomes clear to them that that’s exactly what has happened.”
Dr. David Keegan, MD CCFP(EM) FCFP (2023) ➤
❦ ps.
Escalation of commitment: A human behaviour pattern in which an individual or group facing increasingly negative outcomes from a decision, action, or investment, nevertheless continue the behaviour instead of altering course.
Anon (-10 BC)