📖 Solving the puzzle of Long Covid
‘Reinfection, which is now the dominant type of SARS-CoV-2 infection, is not inconsequential; it can trigger de novo Long Covid or exacerbate its severity.
Each reinfection contributes additional risk of Long Covid: cumulatively, two infections yield a higher risk of Long Covid than one infection, and three infections yield a higher risk than two infections.’
📖 (22 Feb 2024 ~ Science) ‘Solving the puzzle of Long Covid’.
© 2024 Al-Aly & Topol / Science.
❦ Scientific Media Article ~ ‘Solving the puzzle of Long Covid’
By Al-Aly & Topol / Science (22 Feb 2024) [Abridged]
❦ ‘More than 4 years into the global COVID-19 pandemic, widespread infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has left millions of people around the world with Long Covid [Post-Acute Sequelae of COVID-19, or PASC], which describes the constellation of post-acute and long-term adverse health effects caused by the infection.
Evidence generated by the scientific community – with formidable contributions from patient-led research teams – has provided a thorough understanding of the epidemiology and clinical manifestations of Long Covid.
Understanding the biologic underpinnings of this disease is also improving, along with evidence that vaccination and antivirals can help prevent it.
Yet despite this progress, prevention efforts have stalled, there is uncertainty about governments’ long-term commitment to address research needs in this area, and there has yet to be a treatment option validated with randomized controlled trials (RCTs).
‘Long Covid can manifest in people across the life span (from children to older adults) and across race and ethnicity, sex, and baseline health status.
It is a complex non-monolithic, multi-systemic disease with sequelae across almost all organ systems.
The prototypical (classic) form of Long Covid (with brain fog [brain damage], fatigue, dysautonomia, and post-exertional malaise) is more common in younger adults and in females.
Other forms of Long Covid, including those with cardiovascular and metabolic sequelae, are manifest more often in older adults and those with comorbidities.’
In the post-acute phase of COVID-19, there was increased risk of an array of incident neurologic sequelae including:
✺ ischemic and hemorrhagic stroke;
✺ cognition and memory disorders;
✺ peripheral nervous system disorders;
✺ episodic disorders (for example, migraine and seizures);
✺ extrapyramidal and movement disorders;
✺ mental health disorders;
✺ musculoskeletal disorders;
✺ sensory disorders;
✺ Guillain–Barré syndrome;
✺ and encephalitis or encephalopathy.
‘Regardless of age and across the age spectrum, people with COVID-19 had a higher risk of all the neurologic outcomes examined in this analysis.’
A common risk across all types of Long Covid is severity of acute infection; the risk – on the relative scale – increases according to the severity of the acute infection.
‘However, despite the lower relative risk, more than 90% of [Long Covid] cases occur in people who had mild SARS-CoV-2 infection, owing to the much higher prevalence of mild cases.’
Because non-pharmaceutical interventions [NPIs, such as respirator-wearing and air filtration] to reduce the risk of SARS-CoV-2 transmission have largely been abandoned, vaccines are now the primary line of defense against both severe disease in the acute phase of the infection and Long Covid.
Studies have consistently shown that vaccines reduce the risk of Long Covid by 15% to 75%, with a mean of ~40% reduction in risk.
Yet vaccine policies in much of the world restrict boosters to older adults or those with risk factors for severe COVID-19, and with pandemic fatigue, the public’s appetite for boosters seems to be waning.
‘Reinfection, which is now the dominant type of SARS-CoV-2 infection, is not inconsequential; it can trigger de novo Long Covid or exacerbate its severity.
Each reinfection contributes additional risk of Long Covid: cumulatively, two infections yield a higher risk of Long Covid than one infection, and three infections yield a higher risk than two infections.’
Despite this cumulative knowledge on mechanisms, epidemiology, and prevention, there are several major challenges.
Patients are often met with skepticism and dismissal of their symptoms as psychosomatic. The attribution of symptoms to psychological causes has no scientific support; it perpetuates stigma and disenfranchises patients from accessing the care they need.
The lack of consensus on terms, definitions, and clinical trial end points for Long Covid is slowing progress and hampering industry engagement in clinical trials.
Evidence from multiple studies with 2 to 3 years of follow-up indicates prolonged risk for many sequelae and that spontaneous recovery or return to baseline status is uncommon.
Extended follow-up of the 1918 influenza pandemic, poliomyelitis outbreaks, and Epstein-Barr virus [human herpesvirus 4, or HHV-4] infections has demonstrated that new, disabling sequelae of these infections can occur multiple decades later; it is uncertain whether this will also occur with COVID-19.
‘Tied with the anti-science, anti-vaccine movement, a tide of Long Covid denialism is rising.’
This movement sows doubt about the scale and urgency of Long Covid, conflates Long Covid with vaccine-adverse events, and seeks to hamper progress on addressing the care needs of people suffering from this condition.
The pandemic has laid bare a blind spot in epidemiology and surveillance data systems for infectious diseases.
Nearly all surveillance data systems are built on the archaic, and now obsolete, notion that accounting for cases, hospitalization, and death in the acute phase is sufficient to capture the health burden of the infection.
This approach does not account for the burden of long-term health loss due to infectious illnesses, which obscures their true toll. Adding to this challenge are the absent, underdeveloped, or siloed healthcare data systems in much of the world.
Long Covid will have wide-reaching effects that are yet to be fully appreciated.
‘In addition to the prototypical form of Long Covid, SARS-CoV-2 infection increases the risk of a wide array of chronic diseases and will contribute to a rise in the burden of cardiovascular disease, diabetes, neurologic impairment, and autoimmune conditions.’
Long Covid affects the development and educational attainment of children and reduces labor participation and economic productivity in working-age adults.
Both the direct effect of increased risk of death in people with Long Covid, and the indirect effect on mortality through increased burden of chronic diseases caused by SARS-CoV-2 may contribute to further decline in life expectancy, potentially erasing decades of progress.
Finding treatments for Long Covid must be prioritized.
‘Preventing infections and reinfections is the best way to prevent Long Covid and should remain the foundation of public health policy.’
A greater commitment to non-pharmaceutical interventions [NPIs], which include masking [N95/N99, or FFP2/FFP3/P3 respirators], especially in high-risk settings, and improved air quality through filtration and ventilation, are requisite.
Updating building codes to require mitigation against airborne pathogens and ensure safer indoor air should be treated with the same seriousness afforded to mitigation of risks from earthquakes and other natural hazards.
Reducing the risk of serious outcomes after COVID-19 and some prevention of Long Covid can be attained with vaccination of a wider spectrum of the population.
Development of more durable, variant-proof vaccines that are not vulnerable to evasion by the ever-mutating virus needs to be accelerated.
Nasally or orally administered vaccines that induce strong mucosal immunity to block infection and transmission should be pursued.
It is also necessary to broaden the pipeline of SARS-CoV-2 antivirals, especially because of rising resistance.’
❂
📖 (22 Feb 2024 ~ Science) Solving the puzzle of Long Covid: Long Covid provides an opportunity to understand how acute infections cause chronic disease ➤
© 2024 Al-Aly & Topol / Science.
❂
✻ Medical notes:
The neurologic manifestations of Long Covid are hypothesized to be driven by neuro-inflammation with trafficking of immune cells (T cells and natural killer cells), cytokines and antibodies to the brain parenchyma resulting in activation of microglia and astrocytes, disturbances in synaptic signaling of upper-layer excitatory neurons, impaired neurogenesis and neuroblast formation, loss of oligodendrocytes and reduced myelinated axon density.
Other mechanisms may involve endothelial cell injury, complement activation and complement-mediated coagulopathy and microangiopathy leading to microbleeds or microclots.
Evidence from brain lysates of people with COVID-19 (compared with non-infected controls) demonstrates upregulation of transforming-growth-factor-beta signaling, hyperphosphorylation and post-translational modification of receptor and channel proteins typically linked to Alzheimer’s disease.
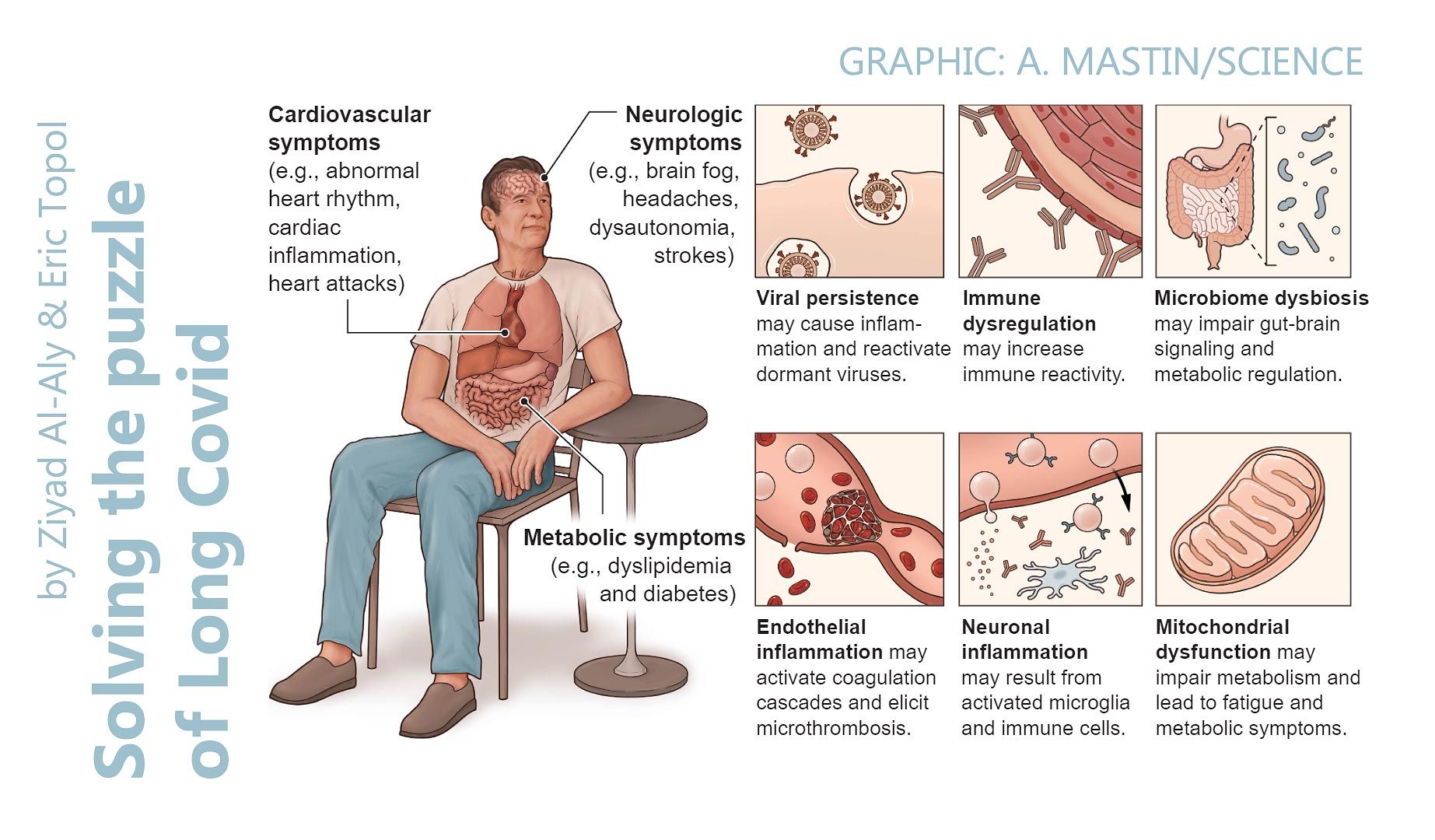
Legend: ‘Long Covid is a multi-systemic disease with sequelae that affect almost all organ systems.’
📖 (22 Feb 2024 ~ Science) Solving the puzzle of Long Covid: Long Covid provides an opportunity to understand how acute infections cause chronic disease ➤
© Graphic: 2024 A. Mastin / Science.
❦ Further Reading on Reinfections
📖 (25 May 2022 ~ Nature Medicine) ‘Long COVID after breakthrough SARS-CoV-2 infection’. ➤
‘At 6 months after infection, beyond the first 30 days of illness, compared to contemporary controls, people with breakthrough SARS-CoV-2 infection (‘BTI’, or reinfection) exhibited a higher risk of death and incident post-acute sequelae, including cardiovascular, coagulation and hematologic, gastrointestinal, kidney, mental health, metabolic, musculoskeletal and neurologic disorders.’
© 2022 Ziyad Al-Aly, Benjamin Bowe & Yan Xie / Nature.
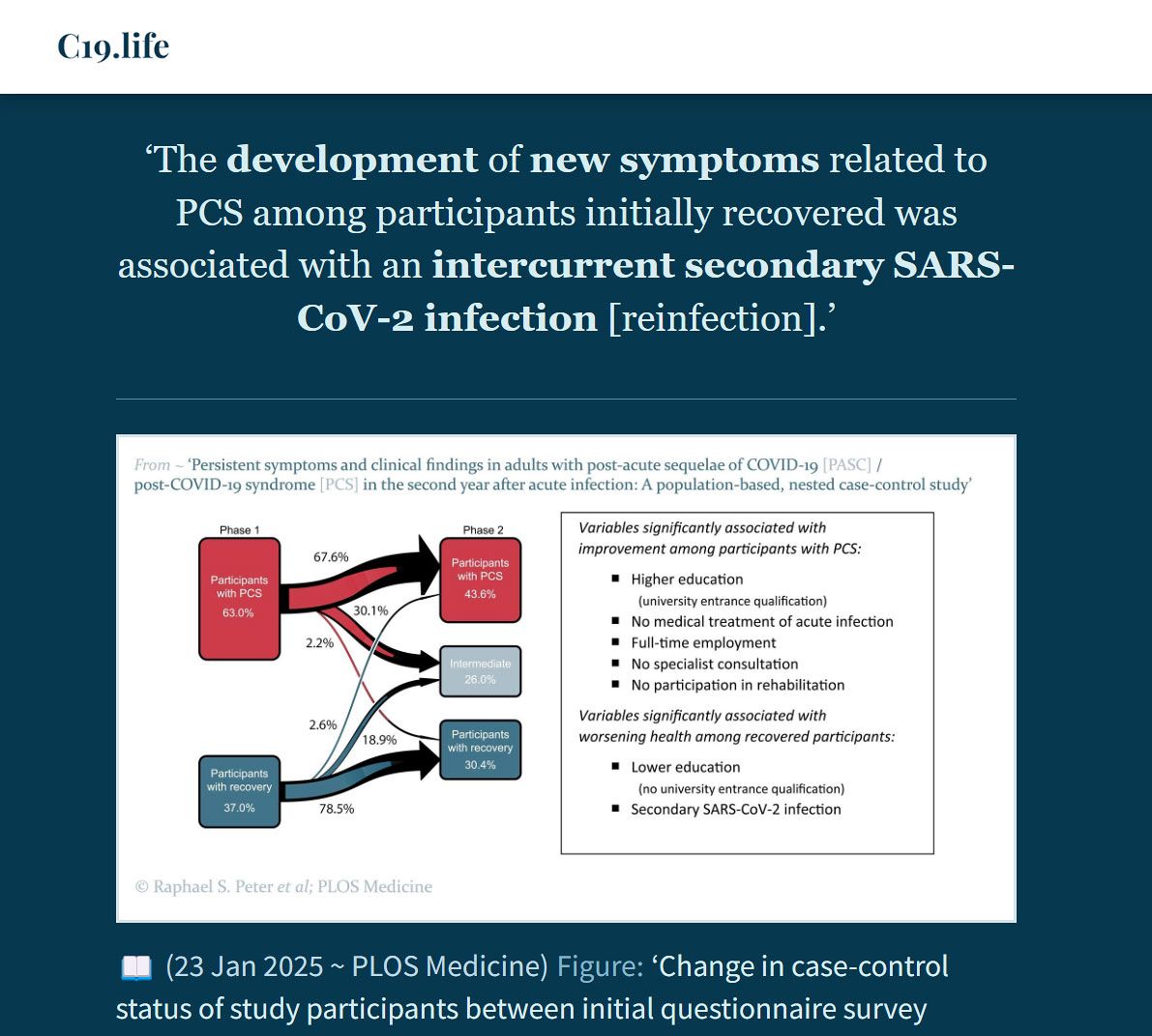
📖 (23 Jan 2025 ~ PLOS Medicine) ‘Persistent symptoms and clinical findings in adults with post-acute sequelae of COVID-19/post-COVID-19 syndrome in the second year after acute infection: A population-based, nested case-control study’. ➲
‘The development of new symptoms related to PCS [Post-COVID-19 Syndrome / ‘Long Covid’] among participants initially recovered was associated with an intercurrent secondary SARS-CoV-2 infection [reinfection].’
© 2025 Raphael S. Peter et al / PLOS Medicine.
More... PCS (PASC / ‘Long Covid’)