Post-exertional malaise (PEM) is a
marked physical or
mental fatigue and
deterioration of
symptoms occurring after
physical,
cognitive,
social or
emotional exertion that would have been tolerated previously.
Symptoms typically worsen
12 to 48 hours after such
activities, and can last for
days,
weeks or
months, making it difficult to manage or predict.
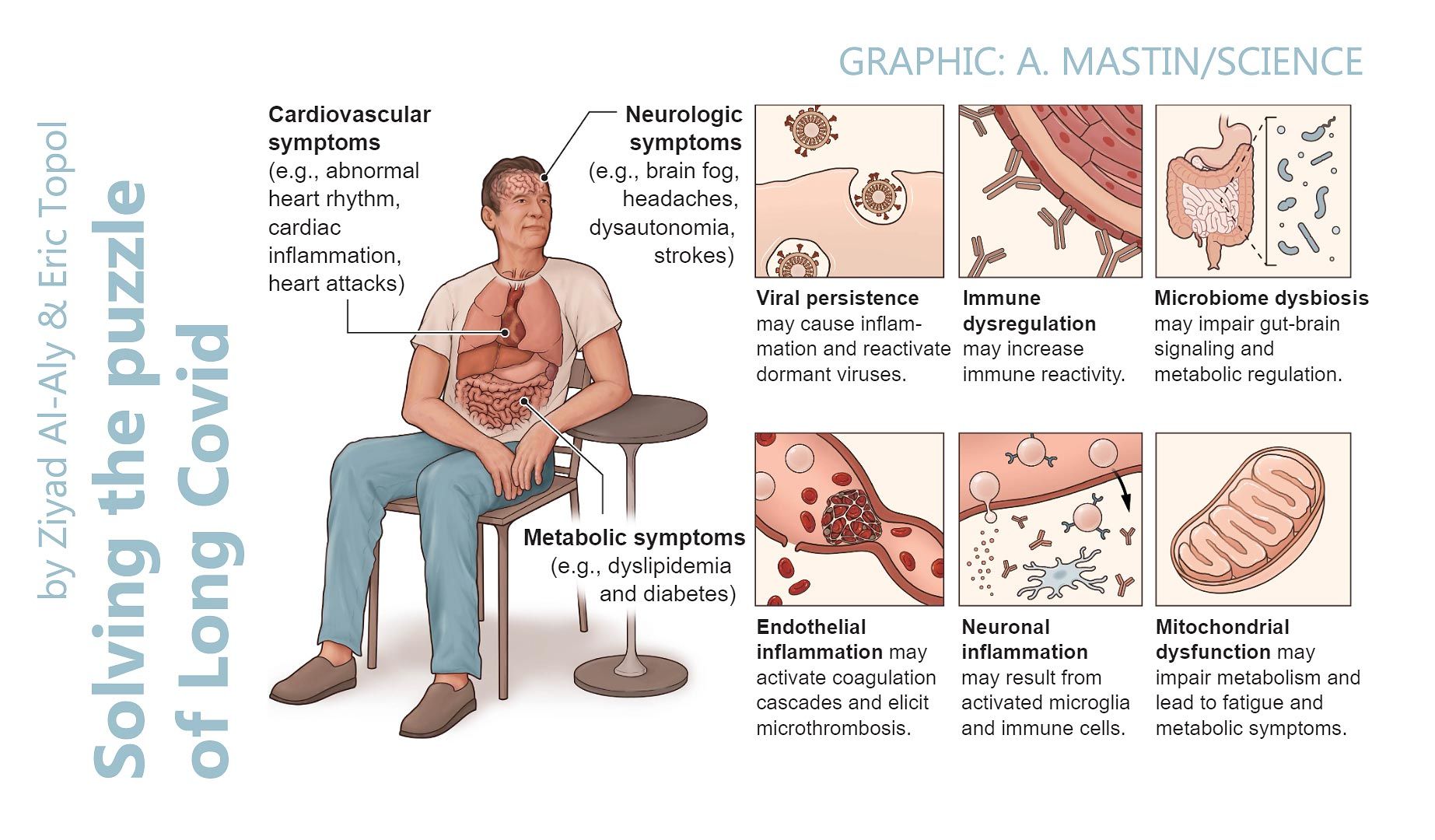
PEM is a hallmark symptom of myalgic encephalomyelitis / chronic fatigue syndrome (ME/CFS), and is commonly reported by people with Post-COVID-19 Syndrome (PCS/‘Long Covid’).
PEM can be
mitigated by
activity management, or ‘pacing’.
📖
(4 Jan 2024 ~ Nature Communications)
‘Muscle abnormalities worsen after post-exertional malaise in long COVID’.
‘A
distinctive symptom of patients with long COVID is
post-exertional malaise, which is associated with a worsening of fatigue- and pain-related symptoms
after acute
mental or
physical exercise.’
📖 (4 Jan 2024 ~ News Medical Life Sciences)
‘Study identifies mitochondrial dysfunction as cause of long-COVID fatigue’.
© 2024
Amsterdam University Medical Center / NewsMedical.net
❦
Scientific Media Article ~
‘Study identifies mitochondrial dysfunction as cause of long-COVID fatigue’
By
Amsterdam University Medical CenterNews
/
News Medical Life Sciences (4 Jan 2024)
❦ ‘Researchers from Amsterdam UMC and Vrije Universiteit Amsterdam (VU) have discovered that the persistent fatigue in patients with long-COVID has a biological cause, namely mitochondria in muscle cells that produce less energy than in healthy patients.
25 long-COVID patients and 21 healthy control participants participated in the study. They were asked to cycle for fifteen minutes. This cycling test caused a long-term worsening of symptoms in people with long-COVID, called post-exertional malaise (PEM).
‘Extreme fatigue occurs after physical, cognitive, or emotional exertion beyond an unknown, individual threshold.’
The researchers looked at the blood and muscle tissue 1 week before the cycling test and 1 day after the test.
“We saw various abnormalities in the muscle tissue of the patients. At the cellular level, we saw that the mitochondria of the muscle, also known as the energy factories of the cell, function less well and that they produce less energy,” says Rob Wüst, Assistant Professor at Department of Human Movement Sciences at the VU University.
“So, the cause of the fatigue is really biological. The brain needs energy to think. Muscles need energy to move. This discovery means we can now start to research an appropriate treatment for those with long-COVID,” adds van Vugt.
One of the theories about long-COVID is that coronavirus particles may remain in the body of people who have had the coronavirus.
“We don’t see any indications of this in the muscles at the moment,” says Van Vugt.
The researchers also saw that the heart and lungs functioned well in the patients. This means that the long-lasting effect on patient’s fitness is not caused by abnormalities in the heart or lungs.
Exercising is not always good for patients with long-COVID.
“In concrete terms, we advise these patients to guard their physical limits and not to exceed them. Think of light exertion that does not lead to worsening of the complaints. Walking is good, or riding an electric bike, to maintain some physical condition. Keep in mind that every patient has a different limit,” says Brent Appelman, researcher at Amsterdam UMC.
“Because symptoms can worsen after physical exertion, some classic forms of rehabilitation and physiotherapy are counterproductive for the recovery of these patients,” van Vugt adds.
Although the majority of people infected with the SARS-CoV-2 virus recover within weeks, a subgroup, estimated to be around one in eight, will get long-COVID.
Symptoms in patients with long-COVID, post-acute sequelae or COVID or post-COVID syndrome (PCS) include severe cognitive problems (‘brain fog’), fatigue, exercise intolerance, autonomic dysregulation, postural orthostatic tachycardia syndrome (POTS), orthostatic intolerance, and worsening of symptoms after PEM.’
📖 (4 Jan 2024 ~ News Medical Life Sciences)
‘Study identifies mitochondrial dysfunction as cause of long-COVID fatigue’.
© 2024
Amsterdam University Medical Center / NewsMedical.net
‘Viral infections can
alter mitochondrial function, and multiple studies have shown that
residual SARS-CoV-2 protein presence is associated with long COVID.’
📖
(4 Jan 2024 ~ Nature Communications)
‘Muscle abnormalities worsen after post-exertional malaise in long COVID’.
© 2024
Appelman
et al
/ Nature.
❦
Study ~
‘Muscle abnormalities worsen after post-exertional malaise in long COVID’
By
Appelman et al
/
Nature: Communications (4 Jan 2024)
❦ ‘A subgroup of patients infected with SARS-CoV-2 remain symptomatic over three months after infection.
A distinctive symptom of patients with long COVID is post-exertional malaise, which is associated with a worsening of fatigue- and pain-related symptoms after acute mental or physical exercise, but its underlying pathophysiology is unclear.
With this longitudinal case-control study, we provide new insights into the pathophysiology of post-exertional malaise in patients with long COVID.
‘Local and systemic metabolic disturbances, severe exercise-induced myopathy, infiltration of amyloid-containing deposits, and immune cells in skeletal muscles of long COVID are key characteristics of post-exertional malaise.’
We show that skeletal muscle structure is associated with a lower exercise capacity in patients, and local and systemic metabolic disturbances, severe exercise-induced myopathy and tissue infiltration of amyloid-containing deposits in skeletal muscles of patients with long COVID worsen after induction of post-exertional malaise.
This study highlights novel pathways that help to understand the pathophysiology of post-exertional malaise in patients suffering from long COVID and other post-infectious diseases.’
© 2024
Appelman
et al
/ Nature.
Figure 1:
‘Lower exercise capacity in patients with long COVID.’
Figure 3:
‘Metabolic and mitochondrial dysfunction in long COVID patients worsens with post-exertional malaise.’
© 2024
Appelman
et al
/ Nature.
❦
How to commit hara-kiri (and knock down a scarecrow) in the field of academia
A little over a year after Appelman
et al’s Nature paper on mytochondrial dysfunction and PEM, Brigitte Ranque (with friends) decides to publish a rebuttal – for they are in the business of
GET and
CBT, and accurate science hurts their bottom line.
A ‘straw man’ is dispatched to
Nature...
📖
(11 Feb 2025
~ Nature Communications) ‘Reply: Muscle abnormalities in Long COVID’ [Ranque et al]
➤
‘The biology of the “kickbacks” (post exertional malaise, PEM) after activity experienced by people with the post-COVID-19 condition (long COVID) is debated. Some specialists believe it is a result of a protective brain response, and others that it is the result of pathophysiology in the muscle itself. Appelman and colleagues report on muscle damage following a maximal effort physical exercise test in patients with PEM with the COVID-19 condition, and these results are interpreted as showing that exercise damages the tissues of people with PEM and should therefore be avoided. However, we believe the data reported do not support this interpretation, as the patients were substantially deconditioned; the physical activity was extreme and biological changes would be expected in anyone; and there were no control patients with a post-COVID-19 condition without PEM. The implications of erroneous interpretation of these data could result in patients fearing that PEM causes physical damage and consequently avoiding approaches to rehabilitation that could help them...’
Etc, etc, etc.
© 2025
Nature Communications.
📖
(11 Feb 2025
~ Nature Communications)
‘Reply: Muscle abnormalities in Long COVID’ [Appelman et al]
➤
‘We thank Ranque et al. for their interest in our recent work and alternative interpretation of our data. We refute that our findings are due to deconditioning, as Long COVID-related skeletal muscle differ fundamentally from those caused by deconditioning. We demonstrated significant physiological differences in Long COVID patients with post-exertional malaise (PEM) compared to healthy controls, even at matched physical activity levels. PEM encompasses a variety of symptoms and not only muscle soreness. Our study did not address the efficacy of exercise training, and we reject misinterpretations that all forms of exercise cause PEM. We advocate further research to define safe exercise thresholds and improve the understanding of PEM.
Ranque et al. state that “everyone can experience severe muscle pain when returning to intense exercise after periods of a few weeks of rest”. Every participant experienced maximal exercise, healthy participants with low fitness also participated, and a proportion of Long COVID patients still possessed fitness levels >50th percentile for their respective sex and age, despite all patients experiencing PEM. Despite several controls having a VO₂ max similar to patients, none reported PEM symptoms...’
Etc.
© 2025
Nature Communications.
✾
More... Post-Exertional Malaise (PEM)
by R. Peter et al / PLOS Medicine
•
23 January 2025
‘The predominant symptoms, often clustering together, remain fatigue, cognitive disturbance and chest symptoms, including breathlessness, with sleep disorder and anxiety as additional complaints. Many patients with persistent PCS [PASC/‘Long Covid’] show impaired executive functioning, reduced cognitive processing speed and reduced physical exercise capacity.’
by Dempsey et al / BMJ Journals ~ Occupational and Environmental Medicine
•
8 October 2024
‘This study included 5248 healthcare workers. While 33.6% reported prolonged COVID-19 symptoms consistent with PCS, only 7.4% reported a formal diagnosis of PCS. Fatigue, difficulty concentrating, insomnia, and anxiety or depression were the most common PCS [Post-COVID-19 Syndrome] symptoms. Baseline risk factors for reporting PCS included screening for common mental disorders, direct contact with COVID-19 patients, pre-existing respiratory illnesses, female sex and older age.’
by Vernon et al / WORK: A Journal of Prevention, Assessment & Rehabilitation
•
7 March 2023
‘Low and medium physical and cognitive exertion triggered PEM for both Long COVID respondents and ME/CFS patients. Long COVID respondents indicated that high physical and cognitive exertion, stress, food or chemical sensitivities, temperature extremes, insufficient sleep, and illness were significantly more likely to trigger PEM than reported by ME/CFS patients.’
More... PASC (PCS / ‘Long Covid’)
by C19.Life... et al
•
21 November 2025
‘Although COVID-19 was originally considered a respiratory illness, it is now well established that SARS-CoV-2 infection can have far-reaching impacts on the nervous system. Common neurological symptoms in Long COVID [PASC] include new-onset cognitive difficulties, dysautonomia, fatigue, and peripheral neuropathy.’ from ‘Neuroimmune pathophysiology of long COVID’ by Moen et al / Psychiatry and Clinical Neurosciences (2025).
by CIDRAP ❂ Cai et al / The Lancet: Infectious Diseases
•
2 April 2025
‘These findings have important implications for understanding the potential impact of COVID-19 on long-term immune function and susceptibility to pathogens.’
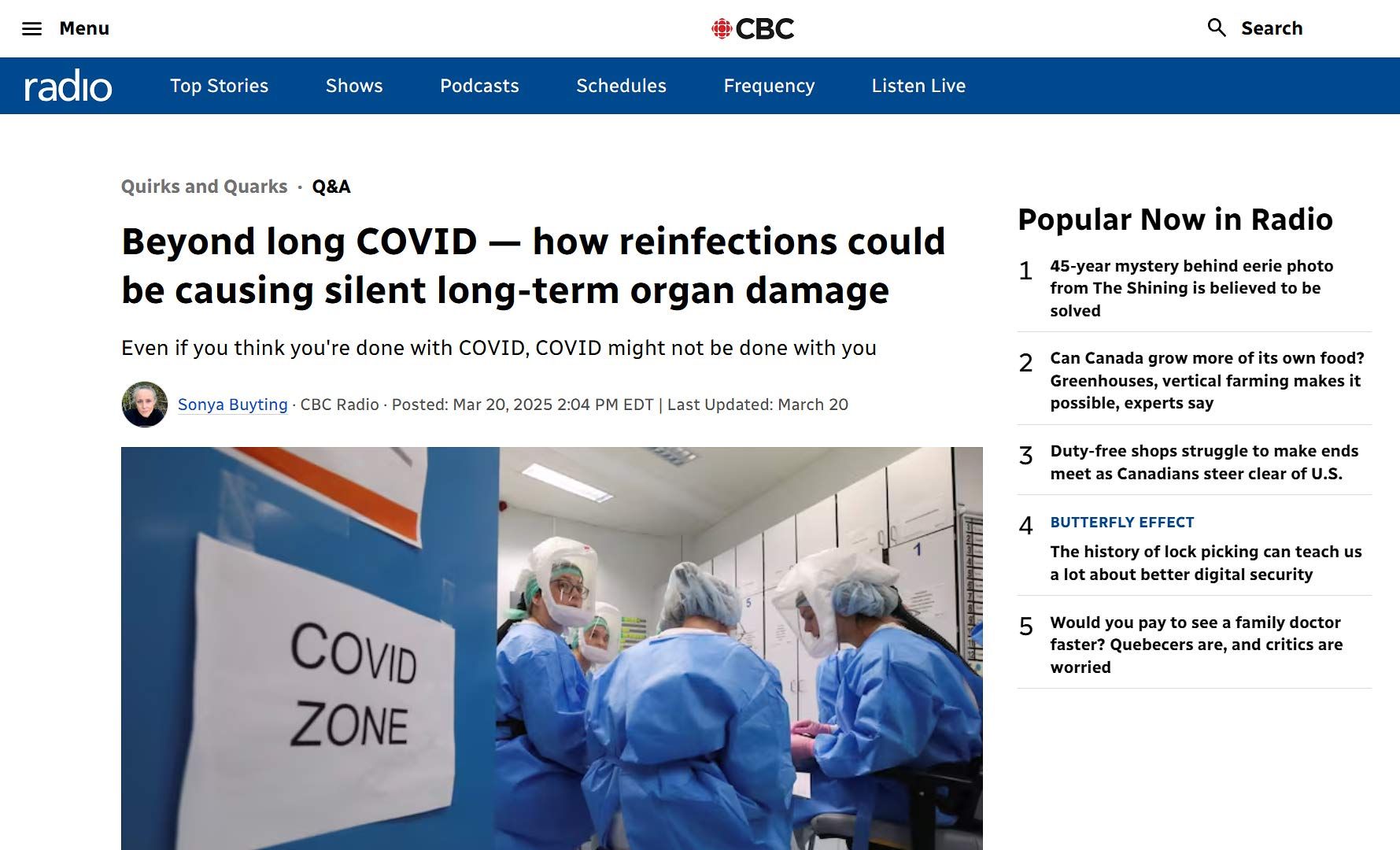
by David Putrino ❂ Sonya Buyting ~ Radio-Canada / Canadian Broadcasting Corporation
•
20 March 2025
CBC Radio-Canada interview with long COVID [PASC] researcher David Putrino from the Icahn School of Medicine at Mount Sinai in New York.
by Jason Gale / Bloomberg UK
•
3 March 2025
‘For patients already battling Alzheimer’s disease, studies indicate that Covid can exacerbate brain inflammation, damage immune cells, and accelerate the disease. Even previously healthy older adults face an increased risk of cognitive impairment and new-onset dementia after infection. Mild Covid cases in younger adults have also been linked to brain issues affecting memory and thinking. ’
by C19.Life... et al
•
28 February 2025
‘But even people who had not been hospitalized had increased risks of many conditions, ranging from an 8% increase in the rate of heart attacks to a 247% increase in the rate of heart inflammation.’ Nature (2 Aug 2022) ‘Either symptomatic or asymptomatic SARS-CoV-2 infection is associated with increased risk of late cardiovascular outcomes and has causal effect on all-cause mortality in a late post-COVID-19 period.’ The American Journal of Cardiology (15 Sep 2023)
by Huang et al / BMC Medicine
•
6 February 2025
‘The proportions of PACS [PASC/Long Covid] patients experiencing chest pain, palpitation, and hypertension as sequelae were 22%, 18%, and 19% respectively.’
by News Medical Life Sciences ❂ Duff et al / Nature Medicine
•
2 February 2025
‘Scientists discover that even mild COVID-19 can alter brain proteins linked to Alzheimer’s disease, potentially increasing dementia risk. COVID-19-positive individuals exhibited lower cognitive test performance compared to controls – equivalent to almost two years of age-related cognitive decline. ’
by R. Peter et al / PLOS Medicine
•
23 January 2025
‘The predominant symptoms, often clustering together, remain fatigue, cognitive disturbance and chest symptoms, including breathlessness, with sleep disorder and anxiety as additional complaints. Many patients with persistent PCS [PASC/‘Long Covid’] show impaired executive functioning, reduced cognitive processing speed and reduced physical exercise capacity.’
by C19.Life
•
16 November 2024
❦ On that 700-day cough... It’s a new thing, but it’s only reserved for inside supermarkets and offices. And pharmacies and hospitals and care homes. Oh, and your living-room. But apart from that, it’s not exactly a deal-breaker. I mean, c’mon. They put up with way worse in the 1900s.
by Porter et al / The Lancet: Regional Health (Americas)
•
23 October 2024
❦ ‘In this population of healthy young adult US Marines with mostly either asymptomatic or mild acute COVID-19, one fourth reported physical , cognitive , or psychiatric long-term sequelae of infection. The Marines affected with PASC [Post-Acute Sequelae of COVID-19 / Post-COVID-19 Complications / ‘Long Covid’] showed evidence of long-term decrease in functional performance suggesting that SARS-CoV-2 infection may negatively affect health for a significant proportion of young adults .’ ❂ ‘Among the 899 participants, 88.8% had a SARS-CoV-2 infection. Almost a quarter (24.7%) of these individuals had at least one COVID-19 symptom that lasted for at least 4 weeks meeting the a priori definition of PASC established for this study. Among those with PASC, 10 had no acute SARS-CoV-2 symptoms after PCR-confirmed infection suggesting that PASC can occur among asymptomatic individuals. Many participants reported that lingering symptoms impaired their productivity at work, caused them to miss work, and/or limited their ability to perform normal duty/activities. Marines with PASC had significantly decreased physical fitness test scores up to approximately one year post-infection with a three-mile run time that averaged in the 65th percentile of the reference cohort. [ PASC was associated with a significantly increased 3-mile run time on the standard Marine fitness test. PASC participants ran 25.1 seconds slower than a pre-pandemic reference cohort composed of 22,612 Marine recruits from 2016 to 2019. A three-mile run evaluates aerobic exercise , overhead lifting of an ammunition can and pull-ups evaluate strength , and shooting a rifle evaluates fine-motor skills .] Scores for events evaluating upper body (pull-ups, crunches, and ammo-can lift) were not significantly reduced by PASC; however, overall physical fitness scores were reduced. ‘The poorer run times and overall scores among PASC participants are indicative of on-going functional effects.’ Standardized health-based assessments for somatization, depression, and anxiety further highlighted the detrimental health effects of PASC. Almost 10% of participants with PASC had PHQ-8 scores ≥10. Increased somatization * has been associated with increased stress, depression, and problems with emotions. * [ Somatization / Somatisation = Medical symptoms caused by psychological stress.] Additionally, PASC participants had higher GAD-7 scores suggesting increased anxiety in a population with unique inherent occupational stressors associated with higher rates of anxiety, depression, and post-traumatic stress disorder. ‘Increased severity of anxiety among those with PASC, combined with greater rates of mental health disorders in general, could portend an ominous combination and should be closely followed.’ Like others, we identified cardiopulmonary symptoms as some of the most prevalent. The high prevalence of symptoms like shortness of breath, difficulty breathing, cough, and fatigue is particularly notable when combined with decreased objective measures of aerobic performance such as running. These results suggest pathology in the cardiopulmonary system. In contrast we observed no reduction in scores assessing strength and marksmanship suggesting the lack of detectable pathology in the neuro-musculoskeletal system. We have previously found in this same cohort that SARS-CoV-2 infection causes prolonged dysregulation of immune cell epigenetic patterns like auto-immune diseases. Based on the reported PASC symptoms, the potential current and future public health implications in this population could be substantial. ‘Chronic health complications from PASC, especially in a young and previously healthy population with a long life expectancy, could decrease work productivity and increase healthcare costs.’ Significant changes in the Years-of-Life lived with a disability can disproportionally increase disability-adjusted life-years, and should be considered when allocating resources and designing policy.’ ❂ 📖 (23 Oct 2024 ~ The Lancet: Regional Health/America) Clinical and functional assessment of SARS-CoV-2 sequelae among young marines – a panel study ➤ © 2024 The Lancet .
by Dempsey et al / BMJ Journals ~ Occupational and Environmental Medicine
•
8 October 2024
‘This study included 5248 healthcare workers. While 33.6% reported prolonged COVID-19 symptoms consistent with PCS, only 7.4% reported a formal diagnosis of PCS. Fatigue, difficulty concentrating, insomnia, and anxiety or depression were the most common PCS [Post-COVID-19 Syndrome] symptoms. Baseline risk factors for reporting PCS included screening for common mental disorders, direct contact with COVID-19 patients, pre-existing respiratory illnesses, female sex and older age.’
by Al-Aly & Topol / Science
•
22 February 2024
‘Reinfection, which is now the dominant type of SARS-CoV-2 infection, is not inconsequential; it can trigger de novo Long Covid or exacerbate its severity. Each reinfection contributes additional risk of Long Covid: cumulatively, two infections yield a higher risk of Long Covid than one infection, and three infections yield a higher risk than two infections.’
by Greene et al / Nature: Neuroscience [Commentary by Danielle Beckman]
•
22 February 2024
❦ “This study confirms everything that I have seen in the microscope over the last few years. The authors of the study use a technique called dynamic contrast-enhanced magnetic resonance imaging ( DCE-MRI ), an imaging technique that can measure the density , integrity , and leakiness of tissue vasculature. Comparing all individuals with previous COVID infection to unaffected controls revealed decreased general brain volume in patients with ‘brain fog’ – along with significantly reduced cerebral white matter volume in both hemispheres in the recovered and ‘brain fog’ cohorts . Covid-19 induces brain-volume loss and leaky blood-brain barrier in some patients. How can this be more clear?” © 2024 Dr. Danielle Beckman, Neuroscientist (PhD Biological Chemistry) ➲ ❂ 📖 (22 Feb 2024 ~ Nature: Neuroscience) Blood–brain barrier disruption and sustained systemic inflammation in individuals with long COVID-associated cognitive impairment ➤ ‘ Our data suggest that sustained systemic inflammation and persistent localized blood-brain barrier (BBB) dysfunction is a key feature of long COVID-associated brain fog. Patients with long COVID had elevated levels of IL-8, GFAP and TGFβ, with TGFβ specifically increased in the cohort with brain fog. GFAP is a robust marker of cerebrovascular damage and is elevated after repetitive head trauma, reflecting BBB disruption, as seen in contact sport athletes and in individuals with self-reported neurological symptoms in long COVID. Interestingly, TGFβ was strongly associated with BBB disruption and structural brain changes. ’ [Layperson overview] 📖 (February 2024 ~ Genetic Engineering and Biotechnology News) Leaky Blood Vessels in the Brain Linked to Brain Fog in Long COVID Patients ➤ [Related] 📖 (7 Feb 2022 ~ Nature: Cardiovascular Research) Blood–brain barrier link to human cognitive impairment and Alzheimer’s disease ➤ ❂
by Meng et al / The Lancet: eClinical Medicine
•
17 February 2024
❦ ‘The occurrences of respiratory disorders among patients who survived for 30 days after the COVID-19 diagnosis continued to rise consistently, including asthma, bronchiectasis, COPD, ILD, PVD*, and lung cancer. * COPD = Chronic obstructive pulmonary disease . ILD = Interstitial lung disease . PVD = Peripheral vascular disease . With the severity of the acute phase of COVID-19, the risk of all respiratory diseases increases progressively. Besides, during the 24-months follow-up, we observed an increasing trend in the risks of asthma and bronchiectasis over time, which indicates that long-term monitoring and meticulous follow-up of these patients is essential. These findings contribute to a more complete understanding of the impact of COVID-19 on the respiratory system and highlight the importance of prevention and early intervention of these respiratory sequelae of COVID-19. In this study, several key findings have been further identified. Firstly, our research demonstrates a significant association between COVID-19 and an increased long-term risk of developing various respiratory diseases. Secondly, we found that the risk of respiratory disease increases with severity in patients with COVID-19, indicating that it is necessary to pay attention to respiratory COVID-19 sequelae in patients, especially those hospitalized during the acute stage of infection. This is consistent with the findings of Lam et al., who found that the risk of some respiratory diseases (including chronic pulmonary disease, acute respiratory distress syndrome and ILD) increased with the severity of COVID-19. Notably, however, our study found that asthma and COPD remained evident even in the non-hospitalized population. This emphasizes that even in cases of mild COVID-19, the healthcare system should remain vigilant. Thirdly, we investigated differences in risk across time periods, as well as the long-term effects of COVID-19 on respiratory disease. During the 2-years follow-up period, the risks of COPD, ILD, PVD and lung cancer decreased, while risks of asthma and bronchiectasis increased. Fourthly, our study showed a significant increase of the long-term risk of developing asthma, COPD, ILD, and lung cancer diseases among individuals who suffered SARS-CoV-2 reinfection. This finding emphasizes the importance of preventing reinfection of COVID-19 in order to protect public health and reduce the potential burden of SARS-CoV-2 reinfection. Interestingly, vaccination appears to have a potentially worsening effect on asthma morbidity compared with other outcomes. This observation aligns with some previous studies that have suggested a possible induction of asthma onset or exacerbation by COVID-19 vaccination. It suggests that more care may be necessary for patients with asthma on taking the COVID vaccines. The underlying mechanisms associated with COVID and respiratory outcomes are not fully understood, but several hypotheses have been proposed. First, SARS-CoV-2 can persist in tissues (including the respiratory tract), as well as the circulating system for an extended period of time after the initial infection. This prolonged presence of the virus could directly contribute to long-term damage of the respiratory tissues, consequently leading to the development of various respiratory diseases. Second, it has been observed that SARS-CoV-2 infection can lead to prolonged immunological dysfunctions, including highly activated innate immune cells, a deficiency in naive T and B cells, and increased expression of interferons and other pro-inflammatory cytokines. These immune system abnormalities are closely associated with common chronic respiratory diseases – asthma, bronchiectasis, COPD, as well as the development of lung cancer. Next, SARS-CoV-2 itself has been shown to drive cross-reactive antibody responses, and a range of autoantibodies were found in patients with COVID-19. In conclusion, our research adds to the existing knowledge regarding the effects of COVID-19 on the respiratory system. Specifically, it shows that the risk of respiratory illness increases with the severity of infection and reinfection. Our findings emphasize the importance of providing extended care and attention to patients previously infected with SARS-CoV-2.’ ❂ 📖 (17 Feb 2024 ~ The Lancet: eClinical Medicine) Long-term risks of respiratory diseases in patients infected with SARS-CoV-2: a longitudinal, population-based cohort study ➤ © 2024 The Lancet: eClinical Medicine .
by Henry Madison
•
9 February 2024
❦ “Chronic disease is like the perfect medical crime. The cause is usually long gone by the time the disease manifests, and nobody links the two until it’s much too late for most.” ❂ © 2024 Henry Madison . ➲
by Dr. David Joffe PhD / FRACP (Respiratory Physician)
•
27 January 2024
❦ “It’s really not in the interest of the virus to kill us quickly. That’s why it has mutated to immune escape. That way it enters silently, and then eats you slowly whilst you’re still a spreading vector. Refrigerator trucks are long gone. That’s all the political class wanted. The unseen costs of CVD [cardiovascular disease] , DM [diabetes mellitus] , and both dementia and Parkinson’s Disease are the train coming down the tunnel. The economists are catching up. The actuaries are already there. Politicians and most people? Not yet...” ❂ © 2024 Dr. David Joffe PhD / FRACP (Respiratory Physician) ➲
by Scardua-Silva et al / Nature: Scientific Reports
•
19 January 2024
❦ ‘Although some studies have shown neuroimaging and neuropsychological alterations in post-COVID-19 patients, fewer combined neuroimaging and neuropsychology evaluations of individuals who presented a mild acute infection. Here we investigated cognitive dysfunction and brain changes in a group of mildly infected individuals. We conducted a cross-sectional study of 97 consecutive subjects ( median age of 41 years ) without current or history of psychiatric symptoms (including anxiety and depression) after a mild infection , with a median of 79 days (and mean of 97 days ) after diagnosis of COVID-19. We performed semi-structured interviews, neurological examinations, 3T-MRI scans, and neuropsychological assessments. The patients reported memory loss ( 36% ), fatigue ( 31% ) and headache ( 29% ). The quantitative analyses confirmed symptoms of fatigue ( 83% of participants), excessive somnolence ( 35% ), impaired phonemic verbal fluency ( 21% ), impaired verbal categorical fluency ( 13% ) and impaired logical memory immediate recall ( 16% ). Our group… presented higher rates of impairments in processing speed ( 11.7% in FDT- Reading and 10% in FDT- Counting ). The white matter (WM) analyses with DTI * revealed higher axial diffusivity values in post-infected patients compared to controls. * Diffusion tensor imaging tractography , or DTI tractography, is an MRI (magnetic resonance imaging) technique most commonly used to provide imaging of the brain. Our results suggest persistent cognitive impairment and subtle white matter abnormalities in individuals mildly infected , without anxiety or depression symptoms. One intriguing fact is that we observed a high proportion of low average performance in our sample of patients (which has a high average level of education ), including immediate and late verbal episodic memory, phonological and semantic verbal fluency, immediate visuospatial episodic memory, processing speed, and inhibitory control . Although most subjects did not present significant impaired scores compared with the normative data, we speculate that the low average performance affecting different domains may result in a negative impact in everyday life , especially in individuals with high levels of education and cognitive demands .’ ❂ ❦ Note how these findings might negatively affect daily activities that demand sustained cognitive attention and fast reaction times – such as driving a car or motorbike, or piloting a plane. Consider air-traffic control. Consider the impact on healthcare workers whose occupations combine long periods of intense concentration with a need for critical precision. ❂ 📖 (19 Jan 2024 ~ Nature: Scientific Reports) Microstructural brain abnormalities, fatigue, and cognitive dysfunction after mild COVID-19 ➤ © 2024 Nature .
by Harris et al / Current Osteoporosis Reports
•
18 January 2024
‘ Clinical evidence suggests that SARS-CoV-2 may lead to hypocalcemia, altered bone turnover markers, and a high prevalence of vertebral fractures. ’
by Wolfram Ruf / Science
•
18 January 2024
❦ ‘Acute infections with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) cause a respiratory illness that can be associated with systemic immune cell activation and inflammation , widespread multi-organ dysfunction , and thrombosis . Not everyone fully recovers from COVID-19, leading to Long Covid, the treatment of which is a major unmet clinical need. Long Covid can affect people of all ages , follows severe as well as mild disease , and involves multiple organs . Patients with Long Covid display signs of immune dysfunction and exhaustion , persistent immune cell activation , and autoimmune antibody production , which are also pathological features of acute COVID-19. The complement system is crucial for innate immune defense by effecting lytic destruction of invading micro-organisms, but when uncontrolled, it causes cell and vascular damage . The complement cascade is activated by antigen–antibody complexes in the classical pathways or in the lectin pathway by multimeric proteins (lectins) that recognize specific carbohydrate structures, which are also found on the SARS-CoV-2 spike protein that facilitates host cell entry. Both pathways may contribute to the pronounced complement activation in acute COVID-19. Long Covid symptoms include a postexertional exhaustion reminiscent of other post-viral illnesses , such as myalgic encephalomyelitis ( ME ) – chronic fatigue syndrome ( MECFS ) with suspected latent viral reactivation . Antibody titer changes in Long Covid patients indicate an association of fatigue with reactivation of latent Epstein-Barr virus ( EBV ) infections , and Cervia-Hasler et al found that the severity of Long Covid symptoms is associated with cytomegalovirus ( CMV ) reactivation . A better understanding of the connections between viral reactivation, persistent interferon signaling, and autoimmune pathologies promises to yield new insights into the thromboinflammation associated with Long Covid. Although therapeutic interventions with coagulation and complement inhibitors in acute COVID-19 produced mixed results, the pathological features specific for Long Covid suggest potential interventions for clinical testing. Microclots are also observed in ME-CFS patients , indicating crucial interactions between complement, vWF, and coagulation-mediated fibrin formation in post-viral syndromes. A better definition of these interactions in preclinical and clinical settings will be crucial for the translation of new therapeutic concepts in chronic thromboinflammatory diseases .’ ❂ 📖 (18 Jan 2024 ~ Science) Immune damage in Long Covid ➤ © 2024 Wolfram Ruf / Science .
by Michael Merschel / American Heart Association
•
16 January 2024
“I would argue that COVID-19 is not a disease of the lungs at all. It seems most likely that it is what we call a vascular and neurologic infection, affecting both nerve endings and our cardiovascular system.”
by Shajahan et al / Frontiers in Aging Neuroscience
•
8 January 2024
‘[COVID-19’s] ability to invade the central nervous system through the hematogenous and neural routes, besides attacking the respiratory system, has the potential to worsen cognitive decline in Alzheimer’s disease patients. The severity of this issue must be highlighted.’
by Carolyn Barber / Fortune & Outbreak Updates
•
14 December 2023
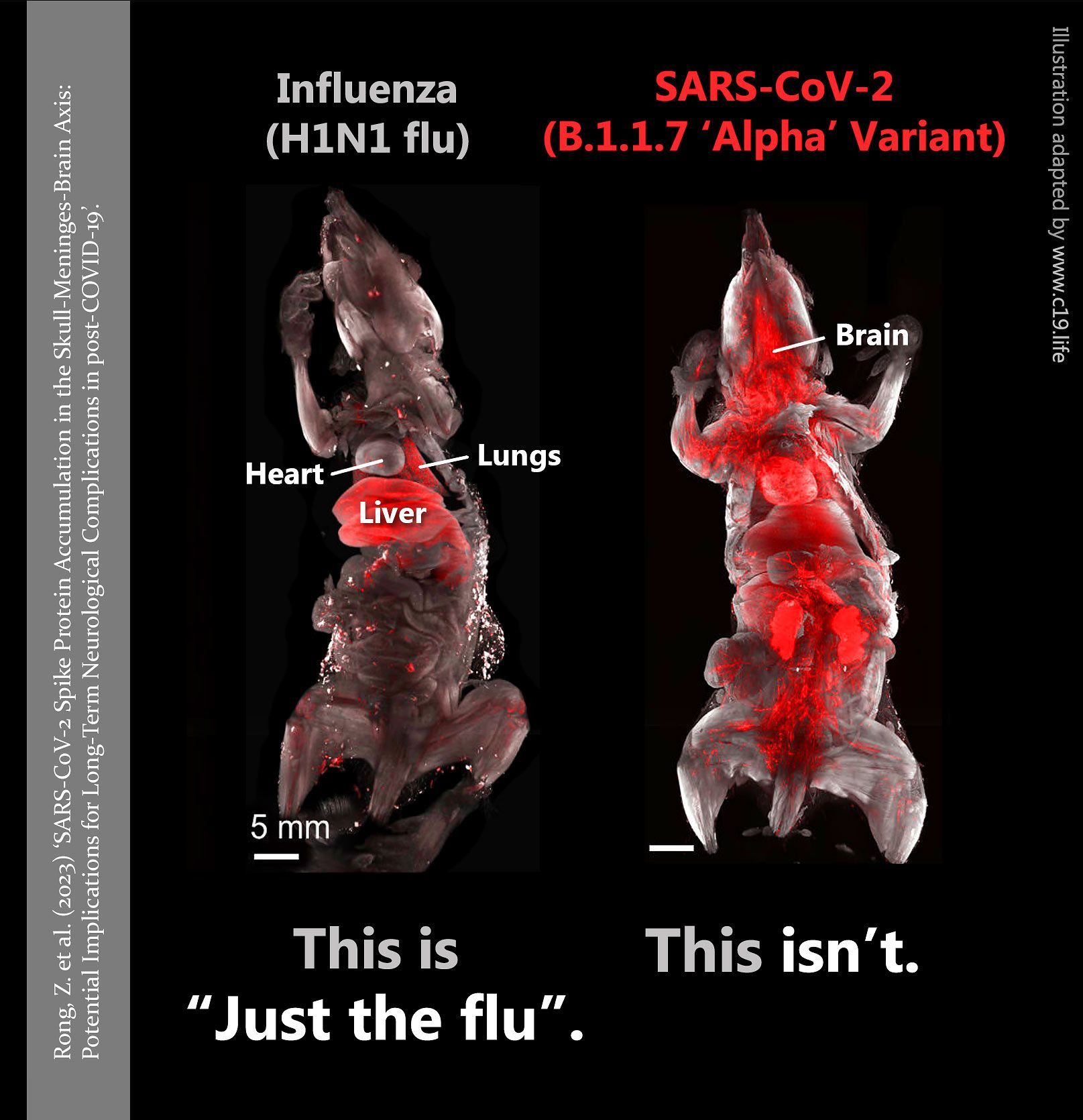
❦ ‘Al-Aly’s study undertook a comparative analysis of 94 pre-specified health outcomes and found that over 18 months of follow-up, COVID was associated with a “ significantly increased risk ” for 64 of them, or nearly 70% . The disease’s enhanced risk list includes everything from cardiac arrest , stroke , chronic kidney disease , and cognitive impairment to mental health and fatigue , characteristics often associated with long COVID. By comparison, the seasonal flu was associated with increased risk in only 6 of the 94 conditions specified. Further, while COVID increased the risks for almost all the organ systems studied, the flu heightened risk primarily for the pulmonary ( lung ) system . Those findings, Al-Aly says, suggest that “ COVID is really a multi-systemic disease , and flu is more a respiratory virus ”.’ ❂ 📖 (14 Dec 2023 ~ Fortune) COVID-19 v. Flu: A ‘much more serious threat,’ new study into long-term risks concludes ➤ 📖 (14 Dec 2023 ~ The Lancet) Long-term outcomes following hospital admission for COVID-19 versus seasonal influenza: a cohort study ➤ © 2023 Carolyn Barber / Fortune .
by Bland et al / Occupational Medicine
•
11 December 2023
❦ ‘As a consequence of their occupation, doctors and other healthcare workers were at higher risk of contracting coronavirus disease 2019 (COVID-19), and more likely to experience severe disease compared to the general population. Post-acute COVID (Long COVID) in UK doctors is a substantial burden. Insufficient respiratory protection could have contributed to occupational disease, with COVID-19 being contracted in the workplace , and resultant post-COVID complications. Although it may be too late to address the perceived determinants of inadequate protection for those already suffering with Long COVID, more investment is needed in rehabilitation and support of those afflicted .’ ❂ 📖 (11 Dec 2023 ~ Occupational Medicine) Post-acute COVID-19 complications in UK doctors: results of a cross-sectional survey ➤
by Pearson-Stuttard et al / The Lancet (Regional Health Europe)
•
1 December 2023
❦ 'For middle-aged adults ( 50–64 ) in this period [June 2022 – June 2023 ], the relative excess for almost all causes of death examined was higher than that seen for all ages .' ➲ ‘Since July 2020, the Office for Health Improvement and Disparities (OHID) has published estimates of excess mortality. In the period from week ending 3rd June 2022 to 30th June 2023 , excess deaths for all causes were relatively greatest for 50–64 year olds ( 15% higher than expected ), compared with 11% higher for 25–49 and < 25 year olds , and about 9% higher for over 65 year old groups. Several causes, including cardiovascular diseases , show a relative excess greater than that seen in deaths from all-causes ( 9% ) over the same period (week ending 3rd June 2022–30th June 2023), namely: all cardiovascular diseases ( 12% ), heart failure ( 20% ), ischaemic heart diseases ( 15% ), liver diseases ( 19%) , acute respiratory infections ( 14% ), and diabetes ( 13% ). For middle-aged adults (50–64) in this 13-month period, the relative excess for almost all causes of death examined was higher than that seen for all ages . Deaths involving cardiovascular diseases were 33% higher than expected, while for specific cardiovascular diseases, deaths involving ischaemic heart diseases were 44% higher , cerebrovascular diseases 40% higher and heart failure 39% higher . Deaths involving acute respiratory infections were 43% higher than expected and for diabetes , deaths were 35% higher . Deaths involving liver diseases were 19% higher than expected for those aged 50–64 , the same as for deaths at all ages. Looking at place of death, from 3rd June 2022 to 30th June 2023 there were 22% more deaths in private homes than expected compared with 10% more in hospitals . The greatest numbers of excess deaths in the acute phase of the pandemic were in older adults. The pattern now is one of persisting excess deaths which are most prominent in relative terms in middle-aged and younger adults , with deaths from CVD [cardiovascular] causes and deaths in private homes being most affected.’ ❂ ➲ [C19.Life Note ] : Considering their findings and conclusion, I’m not sure why the authors would choose to use the term ‘post-pandemic’ in this title – when their evidence points to an on-going pandemic, fueled by continuing high rates of infection, that is now simply killing younger age-groups than previously seen.] ❂ 📖 (1 Dec 2023 ~ The Lancet (Regional Health Europe) Excess mortality in England post Covid-19 pandemic: implications for secondary prevention ➤ © 2023 Pearson-Stuttard et al / The Lancet (Regional Health Europe) .
by Outbreak Updates
•
24 November 2023
❦ SARS-CoV-2 infection precipitates a molecular cascade that reactivates latent viral agents. Infection doesn’t just pass through the body’s defenses but rather reprograms them. It reactivates dormant pathogens and perpetuates a cycle of chronic immune activation. Long COVID sufferers are burdened with a significantly higher prevalence of immune responses to certain DNA viruses – namely, Epstein-Barr Virus (EBV)* and Parvovirus B19 – than those in good health. * Epstein-Barr Virus (EBV) is a common human virus that spreads primarily through saliva. It is a member of the herpes virus family and is found all over the world. Most people will get infected with EBV in their lifetime and will not have any symptoms. Elevated levels of antibodies against these viruses in Long COVID patients not only signal potential viral reactivations. It also suggests a reality where SARS-CoV-2 may be inciting a smoldering activation of chronic viral infections. ❂ 📖 (9 Nov 2023 ~ European Heart Journal) Sequential activation of DNA viruses by the RNA virus SARS-CoV-2 in patients with long COVID syndrome ➤ © 2023 Outbreak Updates ➲
by Martin et al / Journal of Neurology
•
7 November 2023
❦ ‘It is now well established that post-COVID syndrome ( PCS ) represents a serious complication in a substantial number of patients following SARS-CoV-2 infection. PCS is diagnosed when COVID-19-related symptoms persist for more than 3 months. It can occur even after an initially mild to moderate course of infection , and comprises a large variety of symptoms . Around 30% of PCS patients show neurological and neuropsychiatric sequelae , such as fatigue , depressive symptoms , and cognitive dysfunction . These are experienced as particularly debilitating, as they have detrimental effects on daily functioning in PCS patients and hamper a successful return to their jobs. Fatigue is a frequent and one of the most debilitating symptoms in post-COVID syndrome (PCS). Recently, we proposed that fatigue is caused by hypoactivity of the brain’s arousal network and reflected by a reduction of cognitive processing speed . Eighty-eight PCS patients with cognitive complaints and 50 matched healthy controls underwent neuropsychological assessment. Seventy-seven patients were subsequently assessed at 6-month follow-up. Patients showed cognitive slowing indicated by longer reaction times compared to control participants in a simple-response tonic alertness task and in all more complex tasks requiring speeded performance . Reduced alertness correlated with higher fatigue . Alertness dysfunction remained unchanged at 6-month follow-up and the same was true for most attention tasks and cognitive domains .’ ❂ 📖 (7 Nov 2023 ~ Journal of Neurology) Persistent cognitive slowing in post-COVID patients: longitudinal study over 6 months ➤ © 2023 Journal of Neurology .
by Rich Haridy / New Atlas
•
31 October 2023
A layperson-level overview from New Atlas on how all variants of SARS-CoV-2 – the virus that causes COVID-19 – are ‘neuroinvasive’ , meaning that all can infect or enter the brain and the nervous system . (From July 2023 Nature Communications study: ‘Neuroinvasion and anosmia are independent phenomena upon infection with SARS-CoV-2 and its variants’.)
by Outbreak Updates
•
11 October 2023
❦ Your brain is a vast city. The roads (myelin) in this city let cars move efficiently. Oligodendrocytes are the construction workers who maintain these roads. As we age, these workers slow down, causing traffic jams and slower thoughts. Enter SARS-CoV-2, the destructive rioter. It doesn’t just disrupt traffic; it damages the roads and chases away the construction crews. Weeks after the riot, the city still struggles to function, with long-lasting road damages and traffic jams. This is the ‘brain fog’ of post-COVID life. ❂ 📖 (24 Sep 2023 ~ Aging and Disease) Role of Microglia, Decreased Neurogenesis and Oligodendrocyte Depletion in Long COVID-Mediated Brain Impairments ➤ © 2023 Outbreak Updates ➲
by Outbreak Updates
•
10 October 2023
❦ Your lungs are balloons made of the finest silk, allowing them to expand and contract effortlessly with each breath. SARS-CoV-2 is as a needle, puncturing and tearing this delicate fabric. In an attempt to heal, the body patches up the punctures, but instead of the original silk, it uses rough patches. These patches – scarring or fibrosis – make parts of the lung rigid, restricting its once flawless expansion. With each subsequent infection, more patches appear, further suffocating the lung’s true function. The virus doesn’t just infect. It sabotages the very essence of our breath. ❂ 📖 (6 Apr 2022 ~ Annals of Medicine and Surgery) Post COVID-19 pulmonary fibrosis; a meta-analysis study ➤ © 2023 Outbreak Updates ➲
by Merck and Co.
•
16 September 2023
❦ ‘The most common causes of acquired lymphocytopenia include: ➲ Protein-energy undernutrition. ➲ HIV infection. ➲ COVID-19 . ➲ Certain other viral infections. Patients with HIV infection routinely have lymphocytopenia, which arises from destruction of CD4+ T cells infected with the HIV virus. Patients with COVID-19 also frequently have lymphocytopenia ( 35% to 83% of patients ) . Lower lymphocyte counts portend a poor prognosis and an increased likelihood of requiring ICU admission and of dying from the disease. The cause of the lymphocytopenia is not completely understood, but COVID-19 can directly infect lymphocytes, and a cytokine-related apoptosis of the cells is likely. ➲ Lymphocytopenia is most often due to AIDS , and recently COVID-19 , or undernutrition, but it also may be inherited or caused by various infections, drugs, or autoimmune disorders. ➲ Patients have recurrent viral , bacterial , fungal , or parasitic infections .’ ❂ 📖 (Accessed 16 Sep 2023 ~ Merck & Co.) Entry for 'Lymphocytopenia' in Merck Manual ➤ © 2023 Merck & Co .
by Sauve et al / eBioMedicine: Lancet Discovery Science
•
12 September 2023
❦ ‘We have recently demonstrated a causal link between loss of gonadotropin-releasing hormone ( GnRH ), the master molecule regulating reproduction , and cognitive deficits during pathological aging , including Down syndrome and Alzheimer’s disease. Olfactory and cognitive alterations , which persist in some COVID-19 patients, and long-term hypotestosteronaemia in SARS-CoV-2-infected men are also reminiscent of the consequences of deficient GnRH, suggesting that GnRH system neuroinvasion could underlie certain post-COVID symptoms and thus lead to accelerated or exacerbated cognitive decline . We explored the hormonal profile of COVID-19 patients and targets of SARS-CoV-2 infection in post-mortem patient brains and human fetal tissue. We found that persistent hypotestosteronaemia in some men could indeed be of hypothalamic origin , favouring post-COVID cognitive or neurological symptoms , and that changes in testosterone levels and body weight over time were inversely correlated. Infection of olfactory sensory neurons and multifunctional hypothalamic glia called tanycytes highlighted at least two viable neuroinvasion routes . Furthermore, GnRH neurons themselves were dying in all patient brains studied , dramatically reducing GnRH expression. Human fetal olfactory and vomeronasal epithelia , from which GnRH neurons arise, and fetal GnRH neurons also appeared susceptible to infection . Putative GnRH neuron and tanycyte dysfunction following SARS-CoV-2 neuroinvasion could be responsible for serious reproductive , metabolic , and mental health consequences in long-COVID and lead to an increased risk of neurodevelopmental and neurodegenerative pathologies over time in all age groups .’ ❂ 📖 (12 Sep 2023 ~ eBioMedicine: Lancet Discovery Science) Long-COVID cognitive impairments and reproductive hormone deficits in men may stem from GnRH neuronal death ➤ © 2023 eBioMedicine: Lancet Discovery Science .
by Antiviral Marketing
•
11 September 2023
❦ — “I don’t know anyone with Long Covid.” — “Everyone I know is tired.” ❂ © 2023 Antiviral Marketing . ➲
by Di Chiara et al / Acta Paediatrica
•
9 September 2023
❦ Children have largely been unaffected by severe COVID-19 compared to adults, but data suggest that they may have experienced new conditions after developing the disease. We compared 1656 exposed and 1656 unexposed children from 1 February 2020 to 30 November 2021. We found significantly higher risks for some new conditions in exposed children, including mental health issues and neurological problems . The overall excess risk for new-onset conditions after COVID-19 was 78% higher in the exposed than unexposed children. ❂ 📖 (9 Sep 2023 ~ Acta Paediatrica) Comparative study showed that children faced a 78% higher risk of new-onset conditions after they had COVID-19 ➤ © 2023 Di Chiara et al / Acta Paediatrica.
by Parotto et al / The Lancet
•
17 July 2023
❦ ‘Individuals with SARS-CoV-2 infection can develop symptoms that persist well beyond the acute phase of COVID-19 or emerge after the acute phase, lasting for weeks or months after the initial acute illness. The post-acute sequelae of COVID-19 (PASC) , which include physical, cognitive, and mental health impairments, are known collectively as long COVID or post-COVID-19 condition (PCC) . The proportion of patients affected by post-COVID-19 condition might be in the range of 10–30% of those infected with SARS-CoV-2, although understanding of this condition is still evolving. Socio-economic factors are fundamental determinants of health after COVID-19. Individuals from low-income and middle-income countries, those from marginalised communities, and those who are socially disadvantaged are probably disproportionately affected. The post-COVID-19 condition is systemic, affecting various organ systems. PCC results in: an increased use of healthcare resources ; a decreased quality of life ; an increased susceptibility to subsequent viral or bacterial infection ; and leads to heightened vulnerability to perioperative morbidity and mortality for individuals who require a surgical procedure for any (unrelated) indication. With a large and growing global population of survivors of COVID-19, the impact on individuals, healthcare systems, communities, and society is likely to be substantial. At present, there are no specific treatments for post-COVID-19-condition.’ ❂ 📖 (17 July 2023 ~ The Lancet) Post-acute sequelae of COVID-19: understanding and addressing the burden of multisystem manifestations ➤ © 2023 Parotto et al / The Lancet.
by Altmann et al / Nature
•
11 July 2023
❦ ‘Long COVID is the patient-coined term for the disease entity whereby persistent symptoms ensue in a significant proportion of those who have had COVID-19, whether asymptomatic, mild or severe. The disease burden spans from mild symptoms to profound disability, the scale making this a huge, new healthcare challenge. Long COVID will likely be stratified into several more or less discrete entities with potentially distinct pathogenic pathways. The evolving symptom list is extensive, multi-organ, multisystem and relapsing–remitting, including fatigue, breathlessness, neurocognitive effects and dysautonomia. A range of radiological abnormalities in the olfactory bulb, brain, heart, lung and other sites have been observed in individuals with Long COVID. Some body sites indicate the presence of microclots; these and other blood markers of hypercoagulation implicate a likely role of endothelial activation and clotting abnormalities. Diverse auto-antibody (AAB) specificities have been found, as yet without a clear consensus or correlation with symptom clusters. There is support for a role of persistent SARS-CoV-2 reservoirs and/or an effect of Epstein-Barr virus reactivation, and evidence from immune subset changes for broad immune perturbation. The oncoming burden of Long COVID faced by patients, healthcare providers, governments and economies is so large as to be unfathomable, which is possibly why minimal high-level planning is currently allocated to it.’ ❂ 📖 (11 July 2023 ~ Nature Reviews: Immunology) The immunology of long COVID ➤ © 2023 Altmann et al / Nature.
by Dr. Kelly Fearnley, NHS (England)
•
4 July 2023
‘Healthcare workers must be provided with respiratory protection and the air quality in hospitals be monitored and improved through the installation of ventilation systems and air filter units.’ ✾
by NHS Palliative Care Medicine Consultant
•
25 June 2023
❦ “Feeling validated that life is ‘back to normal’ as you see all of those unmasked people around you in restaurants, shops and cinemas? I’ll let you in on a little secret. Those who recognise the risk and who would be masked up aren’t even there. They are busy elsewhere staying healthy. More than 400 million now have Long Covid; a disease from Covid that can impact any organ system, and is proven to cause damage to the brain, heart, lung, kidney, gut, immune and multiple other systems. That’s one in 20 globally. How come you don’t know anyone with it? It’s one of three likely reasons… 1. They have been sick so long that they do what most chronically ill people do when they are asked, “How are you?” They say, “I’m fine”. 2. They don’t recognise the relation of their recent heart attack/memory impairment/new diabetes to their Covid illness in the last year. 3. It’s because they aren’t at that restaurant, movie, theatre, work night out as they don’t fancy worsening their already awful situation with a further infection. Out of sight, out of mind. Even those who know someone with Long Covid will minimise it, as it doesn’t fit with the general narrative that Covid is over. It’s too much cognitive dissonance for most people to handle. Easier to believe that everything’s OK, and it must “just be them being anxious”. It’s not over. I’ll let you in on another special secret; it’s not anxiety. It’s a calm determination to maintain health, in the full knowledge of what Covid can do.” © 2023 NHS Palliative Care Medicine Consultant .
by NHS Medical Consultant
•
25 June 2023
❦ I have seen a disproportionate number of young patients with advanced cancer over the last two years. They used to stand out: now it’s every week. The evidence points to direct Covid-driven mechanisms for rises in cancer risk. Will you hear about it in the news? Of course not. Covid’s over. It’s just anxiety now if you’re thinking about it. Except it’s not. It’ll take years for people to accept this. It’ll be too late. A number of my oncology colleagues have been commenting on how they’ve never seen such aggressively-progressive cancers in all their careers since Covid arrived. I’ve been seeing it as all these patients come to me. It isn’t normal. Alarm bells should be ringing loudly. The evidence: 📖 (22 Mar 2023 ~ Global Journal of Life Sciences and Biological Research) Cancer Related-Genes Enriched in Peripheral Blood Mononuclear Cells (PBMCs) of COVID-19 Patients: A Bioinformatics Study ➤ ‘SARS-CoV-2 can be considered a potential risk factor for increasing the probability of developing cancer.’ Study 1: 📖 (7 Jun 2022 ~ Frontiers in Oncology) SARS-CoV-2 M Protein Facilitates Malignant Transformation of Breast Cancer Cells ➤ ‘Coronavirus disease 2019 (COVID-19) has spread faster due to the emergence of SARS-CoV-2 variants, which carry an increased risk of infecting patients with comorbidities, such as breast cancer.’ Study 2: 📖 (9 Aug 2022 ~ Journal of Infection ) Is SARS-CoV-2 an oncogenic virus? ➤ ‘Gene expression of p53 [tumour suppressor] is downregulated in blood of COVID-19 patients. Downregulation persists at least 24 weeks after infection in long COVID-19 patients. Long-term reduction of p53 could have impact on carcinogenesis.’ 📖 (9 Aug 2022 ~ Journal of Infection) Letter to the editor: Is SARS-CoV-2 an oncogenic virus? ➤ Study 3: 📖 (22 Mar 2023 ~ Global Journal of Life Sciences and Biological Research) Cancer related-genes enriched in peripheral blood mononuclear cells (PBMCs) of COVID-19 patients. A bioinformatics study ➤ ‘Numerous cancer-related genes up-regulated in SARS-CoV-2-infected patients, particularly those genes participating in the cell-cycle regulation or engaged in cellular senescence processes.’ Study 4: 📖 (2 Jun 2023 ~ Biochimie) Possible cancer-causing capacity of COVID-19: Is SARS-CoV-2 an oncogenic agent? ➤ ‘One of the most worrying long-term effects of infection is the potential to induce malignant neoplasms, which will be a major health concern over the coming decades. SARS-CoV-2 infection affects many mechanisms that play a crucial role in cancer onset and progression including cell-cycle regulation, the RAAS system and inflammation / proliferation signaling pathways.’ ❂ Related reading : 📖 (9 Aug 2021 ~ Nature: Scientific Reports) More than 50 Long-term effects of COVID-19: a systematic review and meta-analysis ➤ 📖 (21 Jun 2021 ~ Nature: Scientific Reports) The risk of pancreatic adenocarcinoma following SARS-CoV family infection ➤ 📖 (4 Mar 2021 ~ Nature: Scientific Reports) COVID-19 engages clinical markers for the management of cancer and cancer-relevant regulators of cell proliferation, death, migration, and immune response ➤ 📖 (28 Jan 2021 ~ Nature: Scientific Reports) Meta-analysis of host transcriptional responses to SARS-CoV-2 infection reveals their manifestation in human tumors ➤ 📖 (25 Jan 2010 ~ Nature: Oncogene) Viral epigenome in human tumorigenesis ➤ 📖 (Dec 2006 ~ Yale Journal of Biology and Medicine) Viruses and human cancer ➤ ❂ © 2023 NHS Medical Consultant .
by Martinez-Marmol & Hilliard / Queensland Brain Institute
•
8 June 2023
❦ Researchers at The University of Queensland have discovered viruses such as SARS-CoV-2 can cause brain cells to fuse, initiating malfunctions that lead to chronic neurological symptoms. SARS-CoV-2, the virus that causes COVID-19, has been detected in the brains of people with 'Long COVID' months after their initial infection. "We discovered COVID-19 causes neurons to undergo a cell fusion process, which has not been seen before," Professor Hilliard said. "After neuronal infection with SARS-CoV-2, the spike S protein becomes present in neurons, and once neurons fuse, they don't die." "They either start firing synchronously, or they stop functioning altogether." As an analogy, Professor Hilliard likened the role of neurons to that of wires connecting switches to the lights in a kitchen and a bathroom. "Once fusion takes place, each switch either turns on both the kitchen and bathroom lights at the same time, or neither of them," he said. "It's bad news for the two independent circuits." The discovery offers a potential explanation for persistent neurological effects after a viral infection. "In the current understanding of what happens when a virus enters the brain, there are two outcomes – either cell death or inflammation," Dr Martinez-Marmol said. "But we've shown a third possible outcome, which is neuronal fusion." Dr Martinez-Marmol said numerous viruses cause cell fusion in other tissues, but also infect the nervous system and could be causing the same problem there. "These viruses include HIV, rabies, Japanese encephalitis, measles, herpes simplex virus and Zika virus," he said. “Our research reveals a new mechanism for the neurological events that happen during a viral infection. “This is potentially a major cause of neurological diseases and clinical symptoms that is still unexplored.” ❂ 📖 (7 June 2023 ~ Science Advances) SARS-CoV-2 infection and viral fusogens cause neuronal and glial fusion that compromises neuronal activity ➤ 📖 (8 June 2023 ~ Queensland Brain Institute) COVID-19 can cause brain cells to 'fuse' ➤ © 2023 Martinez-Marmol & Hilliard / Queensland Brain Institute / University of Queensland.
by NHS Palliative Medicine Consultant
•
19 May 2023
❦ “What if Covid has been causing mass cognitive impairment and we are all living in an increasingly stupid society? Mad things could happen with that: imagine if hospitals got rid of masks or people started to believe Covid was just a cold? I know that’s far-fetched, but imagine!” ❂ © 2023 NHS Palliative Medicine Consultant .
by The John Snow Project
•
5 May 2023
❦ Prior to 2020, there were four endemic human coronaviruses – OC43, NL-63, 229E, and HKU1 – which were known to cause 10 to 15 percent of common colds – or the ‘Common Cold Coronaviruses’ (CCCs). From at least the 1970s, we’ve known that infection with these coronaviruses does not lead to lasting protection from reinfection – this is textbook knowledge. CCCs are not just colds – they can cause severe pneumonias, and exhibit a risk profile very similar to SARS-CoV-2 with age. If reinfection really did strengthen immunity against CCCs, then older people would be the least affected – because they would have been regularly infected with diverse variants of these viruses in their past. But that is not the case – and SARS-CoV-2 is not a CCC. SARS-CoV-2 has a wide array of accessory proteins that silence and disrupt our normal immune responses. As we get older, our immune systems start to lose their effectiveness – and we become more susceptible to disease. This process is called immunosenescence . Repeated exposure to a virus like SARS-CoV-2 is fast-tracking more people into immunosenescence at ever-earlier ages, with potentially serious repercussions for their health and longevity. SARS-CoV-2 is a particularly nasty virus that can also trigger the hyperactivation of our own immune systems to cause severe disease. Infection by SARS-CoV-2 has been shown to lead to an increase in autoantibodies and autoimmune disease. Approximately 25 percent of people who develop an autoimmune disease will experience multiple autoimmune syndrome, and will risk a cascade of autoimmune conditions. SARS-CoV-2, like its 2002 predecessor SARS-CoV-1, is both a respiratory and a systemic virus, with an extremely broad cell-type and tissue-tropism covering nearly the whole body. Its ability to infect and do damage to lungs, hearts, kidneys, cardiovascular systems and brains is particularly well-documented. If each subsequent infection results in additional internal organ and immune-system damage, then at some point the damage accumulated – together with the accelerated immune-system aging and normal aging processes – can reasonably be expected to outweigh the protective benefits of immunity developed from previous infections. SARS-CoV-2 reinfects more frequently than influenza or the common cold, infects a wider range of organs, does more damage and seems capable of persisting in a range of organs. So if SARS-CoV-2 behaves like a textbook virus – but does more damage more quickly and more regularly – at what point does the body reach its tipping point? ❂ There are two versions of this article: a 7-minute read in simplified language ; and the full editorial version complete with references, which is an 18-minute-read and aimed towards the medical and scientific communities . ❦ 7-minute primer ~ ‘SARS-CoV-2 and “Textbook” Immunity’ ➤ ❦ Full 18-minute editorial ~ ‘SARS-CoV-2 and “Textbook” Immunity’ ➤ ❂ 📖 (5 May 2023 ~ The John Snow Project) SARS-CoV-2 and "Textbook" Immunity ➤ © 2023 The John Snow Project.
by Costanzo et al / International Journal of Molecular Sciences
•
25 April 2023
❦ ‘Some viruses are known to be associated with the onset of specific cancers. These micro-organisms – oncogenic viruses or oncoviruses – can convert normal cells into cancer cells. Seven oncogenic viruses are known to promote tumorigenesis [tumour creation] in humans: Human papillomavirus (HPV) Hepatitis B and C viruses (HBV, HCV) Epstein-Barr virus (EBV) Human T-cell leukemia virus 1 (HTLV-1) Kaposi sarcoma-associated herpesvirus (KSHV) Merkel cell polyomavirus (MCPyV) Recent research indicates that SARS-CoV-2 infection and COVID-19 progression may predispose recovered patients to cancer onset and accelerate cancer development . This hypothesis is based on the growing evidence regarding the ability of SARS-CoV-2 to modulate oncogenic pathways, promoting chronic low-grade inflammation and causing tissue damage.’ ❂ 📖 (25 Apr 2023 ~ International Journal of Molecular Sciences) Deciphering the Relationship between SARS-CoV-2 and Cancer ➤ © 2023 Costanzo et al / International Journal of Molecular Sciences.
by Negm et al / BMC Infectious Diseases
•
23 April 2023
❦ Critically ill COVID-19 patients are highly susceptible to opportunistic fungal infection due to many factors, including virus-induced immune dysregulation , host-related comorbidities, overuse and misuse of antibiotics or corticosteroids, immune modulator drugs, and the emergencies caused by the pandemic. Fungal coinfection is a common complication of critically ill COVID-19 patients admitted to the ICU. Candidiasis , aspergillosis , and mucormycosis are the most common COVID-19-associated fungal infections and have a great impact on mortality rates . ❂ 📖 (18 Apr 2023 ~ BMC Infectious Diseases) Fungal infection profile in critically ill COVID-19 patients: a prospective study at a large teaching hospital in a middle-income country ➤ © 2023 Negm et al / BMC Infectious Diseases.
by Herrera et al / Nature: Scientific Reports
•
19 April 2023
❦ The results presented here reveal that at least 85% [of the 214 patients with post COVID-19 syndrome] exhibit deficits in one neuropsychological test . Also, the youngest patients were those who showed the most marked and heterogeneous cognitive impairment , while the oldest patients maintained their cognitive functions preserved to a greater extent with only a mild impairment in attention and speed processing. ❂ 📖 (19 Apr 2023 ~ Nature: Scientific Reports) Cognitive impairment in young adults with post COVID-19 syndrome ➤ © 2023 Herrera et al / Nature.
by Sayyadi et al / Annals of Hematology
•
19 April 2023
❦ ‘COVID-19 patients have a hypercoagulability state, and thrombosis is a life-threatening complication of them.’ ✻ Hypercoagulability , also known as thrombophilia , is a condition in which there is an abnormally increased tendency towards blood clotting . ‘From the early days of the severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) outbreak to the present, clinical and basic studies have indicated that coronavirus disease 2019 (COVID-19) may be associated with coagulopathy ( CAC ), which is involved in its related morbidity and mortality. Deep vein thrombosis ( DVT ) and pulmonary embolism ( PE ) are common in COVID-19 patients and are remarkably high in the intensive care unit (ICU)–admitted patients. CAC can lead to the formation of circulating microthrombi and macrothrombi which can involve multiple sites, including the lungs , brain , heart , and visceral organs like kidneys and spleen . There is a close relationship between the immune system and coagulation. The components of the hemostatic system play a role in the body’s immunity, and the activation of the immune system strongly influences the hemostatic system. Abnormal activation of the immune system may promote the growth of pathologies associated with thrombosis. COVID-19 is accompanied by an immune-cell hyperactivation and excessive production of proinflammatory cytokines , known as “ cytokine storm ”. CAC is theorized to result from dysregulated interactions between the immune and coagulation systems .’ ❂ 📖 (19 Apr 2023 ~ Annals of Hematology) Status of major hemostatic components in the setting of COVID-19: the effect on endothelium, platelets, coagulation factors, fibrinolytic system, and complement ➤ © 2023 Annals of Hematology .
by Chen et al / Journal of Medical Virology
•
18 April 2023
❦ 'The risk of herpes zoster (HZ) [ shingles ] remained significantly higher [ +60% ] in patients with COVID-19, compared with those without COVID-19. The higher risk of HZ in the COVID-19 cohort compared with that in the non-COVID-19 cohort remained consistent across subgroup analyses regardless of vaccine status, age, or sex. The risk of HZ within a 12-month follow-up period was significantly higher in patients who had recovered from COVID-19 compared with that in the control group.' ❂ 📖 (18 Apr 2023 ~ Journal of Medical Virology) Long-term risk of herpes zoster following COVID-19: A retrospective cohort study of 2 442 686 patients ➤ © 2023 Journal of Medical Virology.
by Wang et al / International Journal of Molecular Sciences
•
18 April 2023
❦ ‘Pulmonary arterial hypertension (PAH) is a pulmonary vascular disease characterized by the progressive elevation of pulmonary arterial pressures.’ Pulmonary Arterial Hypertension ( PAH ) is a progressive lung disease that affects the heart and lungs . It is caused when the tiny arteries in the lungs become thickened and narrowed , causing abnormally high blood pressure in the pulmonary artery . Symptoms include shortness of breath during exercise, fainting spells , dizziness , swelling of the ankles or legs , chest pain , and a racing pulse . ‘It is becoming increasingly apparent that inflammation contributes to the pathogenesis and progression of PAH. Several viruses are known to cause pulmonary arterial hypertension (PAH) , such as SARS-CoV-2 , Human Endogenous Retrovirus K (HERV-K), and Human Immunodeficiency Virus ( HIV ), in part due to acute and chronic inflammation .’ ❂ 📖 (18 Apr 2023 ~ International Journal of Molecular Sciences) Human Endogenous Retrovirus, SARS-CoV-2, and HIV Promote PAH via Inflammation and Growth Stimulation ➤ © 2023 International Journal of Molecular Sciences .
by Sharma & Jagadeesh / Nature Reviews: Rheumatology
•
12 April 2023
❦ The full picture of post-COVID-19 autoimmune diseases and their prevalence is lacking despite numerous case reports and small series. Two studies that use large cohorts now highlight that SARS-CoV-2 infection is linked to a substantially increased risk of developing a diverse spectrum of new-onset autoimmune diseases . The reports by Chang et al and Tesch et al provide a comprehensive overview of diverse new-onset autoimmune conditions after COVID-19. In addition, an earlier preprint of a retrospective matched cohort analysis using data from the Clinical Practice Research Datalink Aurum database of 458,147 SARS-CoV-2-infected and 1,818,929 uninfected adults across England between 31 January 2020 and 30 June 2021 reported that the incidence of type 1 diabetes mellitus , inflammatory bowel disease and psoriasis are significantly associated with SARS-CoV-2 infection. Some of the earliest evidence that SARS-CoV-2 infection leads to dysregulated immune responses came from paediatric patients who presented with multisystem inflammatory syndrome in children (MIS-C) , which, as the name indicates, involves diffuse organ system involvement and a clinical spectrum that overlaps with other hyperinflammatory syndromes , such as Kawasaki disease , toxic-shock syndrome , and macrophage activation syndrome . Since the start of the pandemic, many researchers have also reported isolated cases of adults with various post-COVID-19 autoimmune conditions. ❂ 📖 (12 Apr 2023 ~ Nature Reviews: Rheumatology) High risk of autoimmune diseases after COVID-19 ➤ © 2023 Sharma & Jagadeesh / Nature.
by Linseman Laboratory / University of Denver
•
4 April 2023
❦ The Linseman Laboratory is studying the long-term brain health effects of COVID-19 in individuals with and without traumatic brain injury (TBI). Preliminary data suggest that those with a history of both COVID-19 and TBI experience more severe Long COVID symptoms, a higher symptom burden , and more frequent symptoms . Those who reported having COVID-19 and TBI reported worse depressive symptoms , worse functional outcomes , and increased fatigue . ❂ 📖 (4 Apr 2023 ~ SciTechDaily) Researchers Discover Connection Between Traumatic Brain Injury and Long COVID ➤ © 2023 Linesman Laboratory / University of Denver / SciTechDaily.
by Dr. Kevin Kavanagh, MD / Infection Control Today
•
31 March 2023
‘We are entering a phase of long COVID and chronic disability.’ ❂ ❦ ‘As the numbers of hospitalizations and deaths are dropping, many individuals declare the pandemic all but over, comforted by the belief that infections are mild and less dangerous than the seasonal flu. However, the scientific literature these last few weeks has been filled with deeply concerning reports. We are entering a phase of long COVID and chronic disability. The number of COVID-19 cases in the United States is unknown since our case reporting system has become unreliable and substantially undercounts cases. In England, as of the week ending March 7, 2023, 1 in 40 people is positive for COVID-19 , and reinfections are frequently occurring. It is estimated that as of November 9, 2022, 94% of the U.S. population has been infected by SARS-CoV-2 , and 65% of the United States population has been infected multiple times . The odds of self-reported long COVID were 28% less after the second infection. Unfortunately, the damage of long COVID from a second infection adds to the first . One of the most concerning long-term effects of COVID-19 is immune dysfunction or hypofunction . Confirmatory research was reported this week, and summarized in a National Institute of Health news release which stated: ‘… findings suggest that SARS-CoV-2 infection damages the CD8⁺ T cell response , an effect akin to that observed in earlier studies showing long-term damage to the immune system after infection with viruses such as hepatitis C or HIV .’ The authors conclude that this dysfunction causes lasting damage and may ‘contribute to long COVID, perhaps rendering patients unable to respond robustly to subsequent infections by SARS-CoV-2 variants or other pathogens .’ * * 📖 (20 Mar 2023 ~ National Institutes for Health) SARS-CoV-2 infection weakens immune-cell response to vaccination ➤ These findings mirror those reported by Files et al who state: ‘Overall, expression of these activation and exhaustion markers indicated more severe immune dysregulation of CD8 ⁺ T cells in the hospitalized group.’ And they found that ‘ CD8⁺ T cell expression of exhaustion markers increased in non-hospitalized individuals over time ’. * * 📖 (4 Jan 2021 ~ Journal of Clinical Investigation) Sustained cellular immune dysregulation in individuals recovering from SARS-CoV-2 infection ➤ The authors’ finding of damage to the immune system “akin” to HIV is very concerning, as is the amplification of this result in the NIH news release. Infection Control Today previously reported that the probable cause of the surges in infections we are seeing is an immune dysfunction caused by COVID-19 . With minimal public health interventions, Sweden also experienced surges in respiratory syncytial virus (RSV) cases. Most recently, Sweden has undergone a significant surge in seasonal flu, with reports from the Public Health Agency of Sweden of unusually severe cases. These [Swedish influenza] cases have occurred in ‘... people under the age of 18 without underlying disease or condition, and have been very seriously ill with complications such as myocarditis or encephalitis.’ Other diseases are also rising , exemplified by reports of record-high severe Streptococcal infections and Candida auris . These spikes in infections caused by multiple pathogens are associated with the SARS-CoV-2 pandemic and the mounting evidence of post-COVID-19 immune dysfunction. Vaccinations can not only reduce the incidence of severe disease, but can also help to prevent long COVID, reducing the incidence by 30% to 40%. However, we have expressed concern regarding the bivalent booster’s effectiveness, and reported a rapid waning of booster-induced immunity in the elderly. [See Footnote.] Recently, researchers from the United States found that the relative bivalent booster effectiveness at 5 to 7 months in preventing hospitalizations relative to monovalent vaccine dosages (2, 3, or 4) was 42% and 59% compared to no vaccination. Using the third vaccine dose as a baseline, the UK Health Security Agency found that an additional (fourth) vaccine dosage had effectiveness against hospitalizations at 10 weeks of only 50% .’ Source: 📖 (21 Mar 2023 ~ Infection Control Today) COVID-19: Study Suggests Long-term Damage to Immune System ➤ ❂ Footnote: On waning vaccine effectiveness * ‘Vaccine effectiveness is an important point. Although much of the younger population received a get-out-of-hospital free card for the latest variant, senior citizens were in its crosshairs. During the last 6 months (since May of 2022), those over the age of 75 had a higher rate of hospitalizations than in the Delta surge; those between the ages of 65 and 75 had approximately the same. Both age groups continue to be at high risk for death and disability. However, data showed that for those 65 years of age and older, the monovalent vaccine’s (2 or more doses) effectiveness for preventing hospitalizations fell to 28% in less than a year. Results were worse for those individuals under 65 years – only 19%.’ * 📖 (24 Feb 2023 ~ Infection Control Today) How Soon Is Another Booster Needed? Durability of Vaccine-Induced Immunity ➤ ❂ © 2023 Infection Control Today . ➲